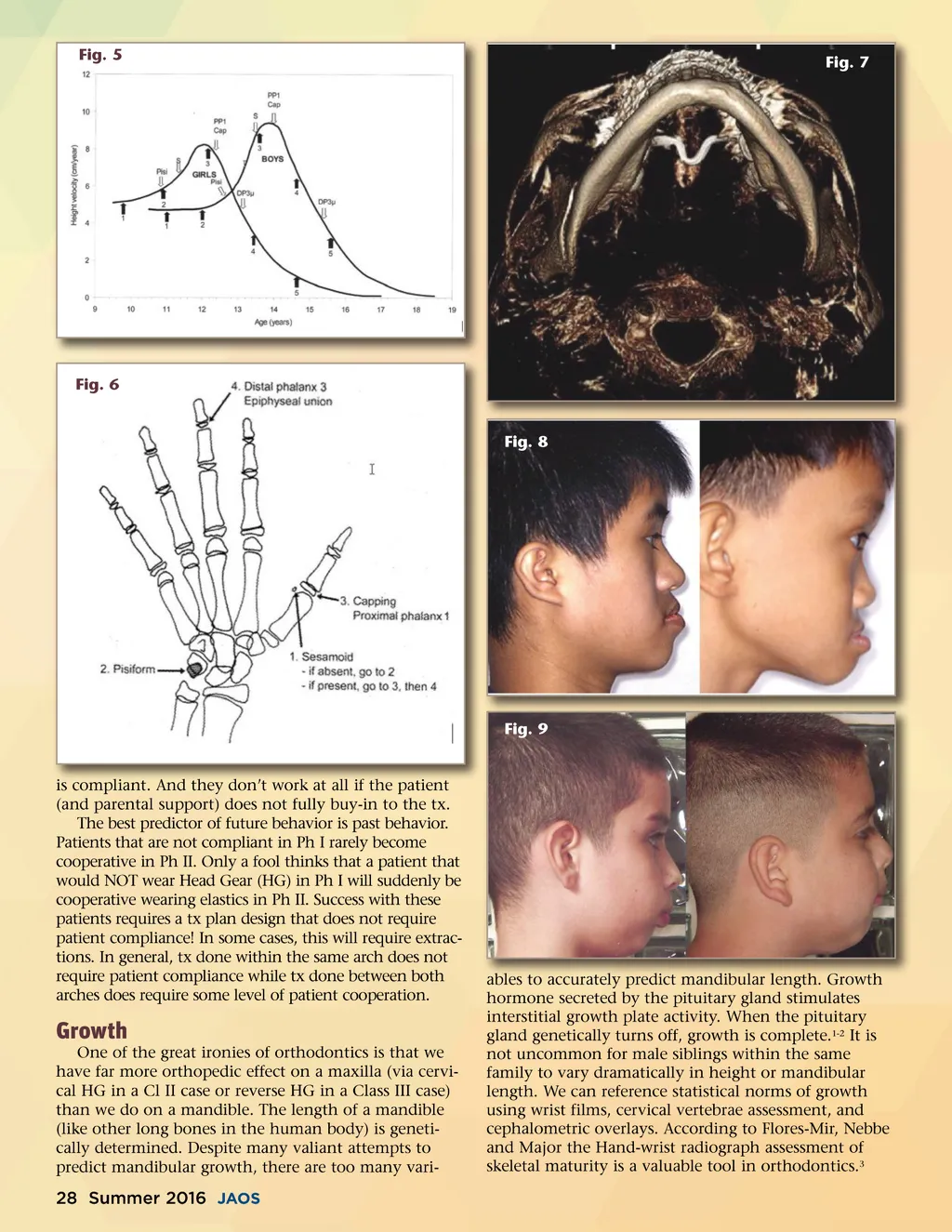
Fig. 5 Fig. 7 Fig. 6 Fig. 8 Fig. 9 is compliant. And they don’t work at all if the patient (and parental support) does not fully buy-in to the tx. The best predictor of future behavior is past behavior. Patients that are not compliant in Ph I rarely become cooperative in Ph II. Only a fool thinks that a patient that would NOT wear Head Gear (HG) in Ph I will suddenly be cooperative wearing elastics in Ph II. Success with these patients requires a tx plan design that does not require patient compliance! In some cases, this will require extrac-tions. In general, tx done within the same arch does not require patient compliance while tx done between both arches does require some level of patient cooperation. Growth One of the great ironies of orthodontics is that we have far more orthopedic effect on a maxilla (via cervi-cal HG in a Cl II case or reverse HG in a Class III case) than we do on a mandible. The length of a mandible (like other long bones in the human body) is geneti-cally determined. Despite many valiant attempts to predict mandibular growth, there are too many vari-ables to accurately predict mandibular length. Growth hormone secreted by the pituitary gland stimulates interstitial growth plate activity. When the pituitary gland genetically turns off, growth is complete. 1-2 It is not uncommon for male siblings within the same family to vary dramatically in height or mandibular length. We can reference statistical norms of growth using wrist films, cervical vertebrae assessment, and cephalometric overlays. According to Flores-Mir, Nebbe and Major the Hand-wrist radiograph assessment of skeletal maturity is a valuable tool in orthodontics. 3 28 Summer 2016 JAOS
Journal of the American Orthodontic Society Summer 2016 / Buyer's Guide: Page 28