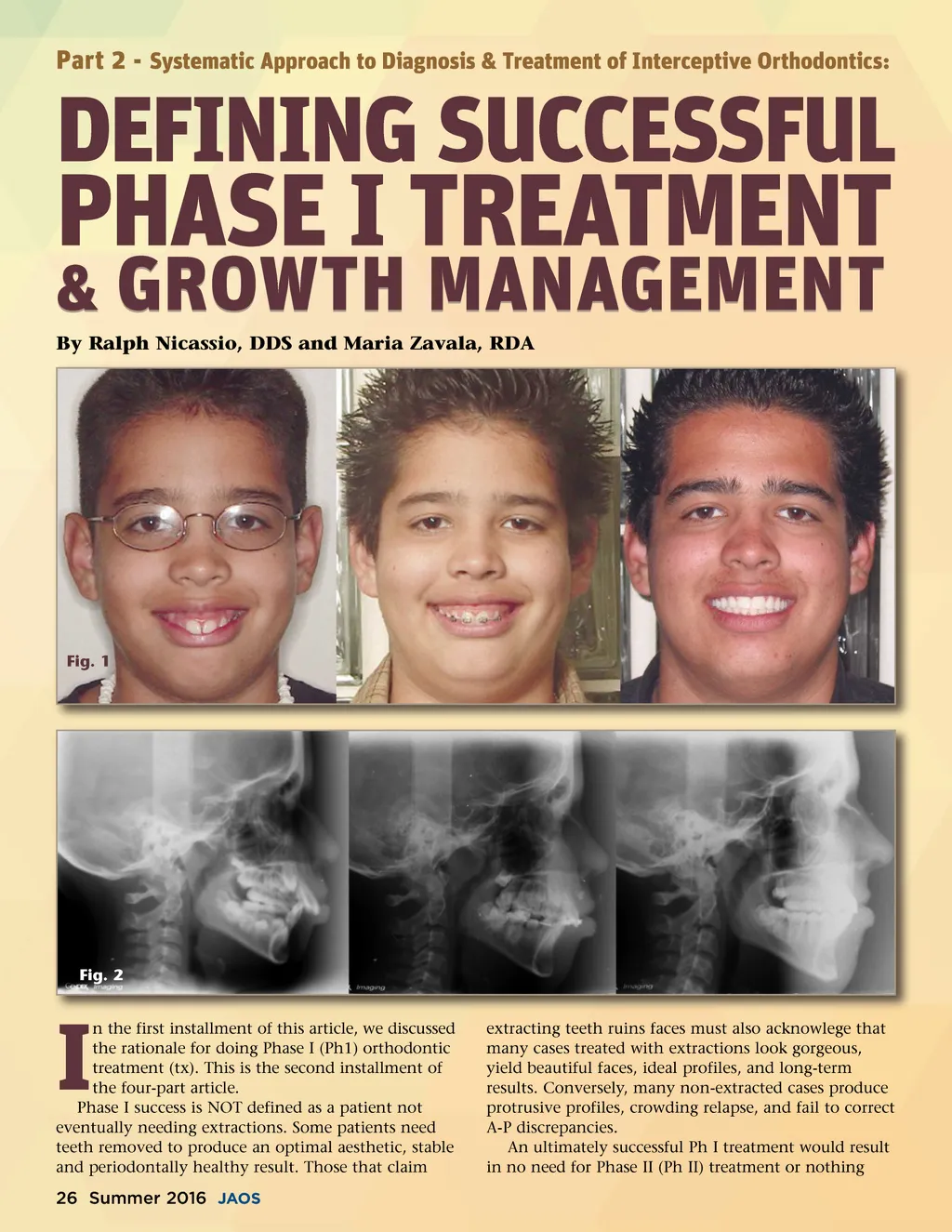
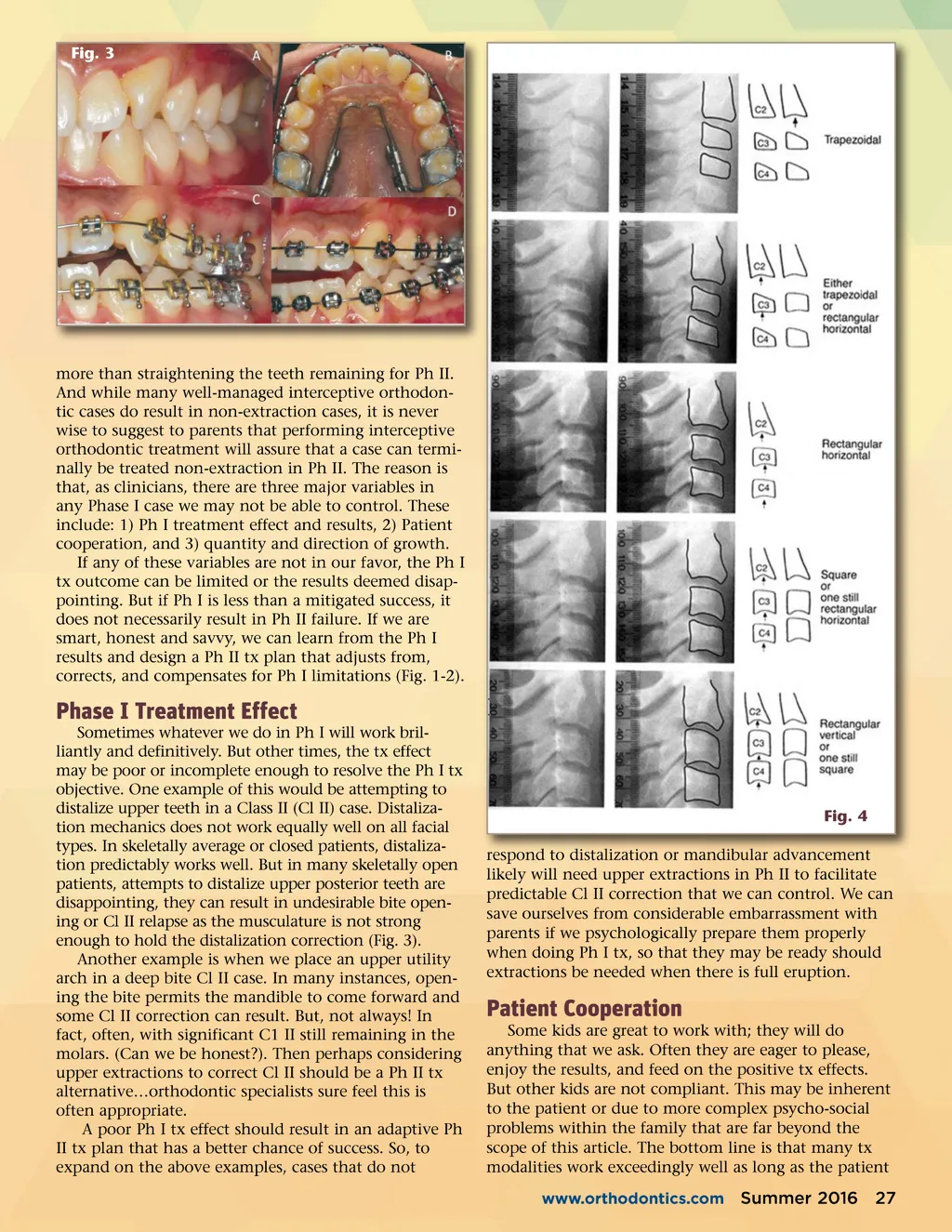
Fig. 3 more than straightening the teeth remaining for Ph II. And while many well-managed interceptive orthodon-tic cases do result in non-extraction cases, it is never wise to suggest to parents that performing interceptive orthodontic treatment will assure that a case can termi-nally be treated non-extraction in Ph II. The reason is that, as clinicians, there are three major variables in any Phase I case we may not be able to control. These include: 1) Ph I treatment effect and results, 2) Patient cooperation, and 3) quantity and direction of growth. If any of these variables are not in our favor, the Ph I tx outcome can be limited or the results deemed disap-pointing. But if Ph I is less than a mitigated success, it does not necessarily result in Ph II failure. If we are smart, honest and savvy, we can learn from the Ph I results and design a Ph II tx plan that adjusts from, corrects, and compensates for Ph I limitations (Fig. 1-2). Phase I Treatment Effect Sometimes whatever we do in Ph I will work bril-liantly and definitively. But other times, the tx effect may be poor or incomplete enough to resolve the Ph I tx objective. One example of this would be attempting to distalize upper teeth in a Class II (Cl II) case. Distaliza-tion mechanics does not work equally well on all facial types. In skeletally average or closed patients, distaliza-tion predictably works well. But in many skeletally open patients, attempts to distalize upper posterior teeth are disappointing, they can result in undesirable bite open-ing or Cl II relapse as the musculature is not strong enough to hold the distalization correction (Fig. 3). Another example is when we place an upper utility arch in a deep bite Cl II case. In many instances, open-ing the bite permits the mandible to come forward and some Cl II correction can result. But, not always! In fact, often, with significant C1 II still remaining in the molars. (Can we be honest?). Then perhaps considering upper extractions to correct Cl II should be a Ph II tx alternative…orthodontic specialists sure feel this is often appropriate. A poor Ph I tx effect should result in an adaptive Ph II tx plan that has a better chance of success. So, to expand on the above examples, cases that do not Fig. 4 respond to distalization or mandibular advancement likely will need upper extractions in Ph II to facilitate predictable Cl II correction that we can control. We can save ourselves from considerable embarrassment with parents if we psychologically prepare them properly when doing Ph I tx, so that they may be ready should extractions be needed when there is full eruption. Patient Cooperation Some kids are great to work with; they will do anything that we ask. Often they are eager to please, enjoy the results, and feed on the positive tx effects. But other kids are not compliant. This may be inherent to the patient or due to more complex psycho-social problems within the family that are far beyond the scope of this article. The bottom line is that many tx modalities work exceedingly well as long as the patient www.orthodontics.com Summer 2016 27
Journal of the American Orthodontic Society Summer 2016 / Buyer's Guide: Page 27