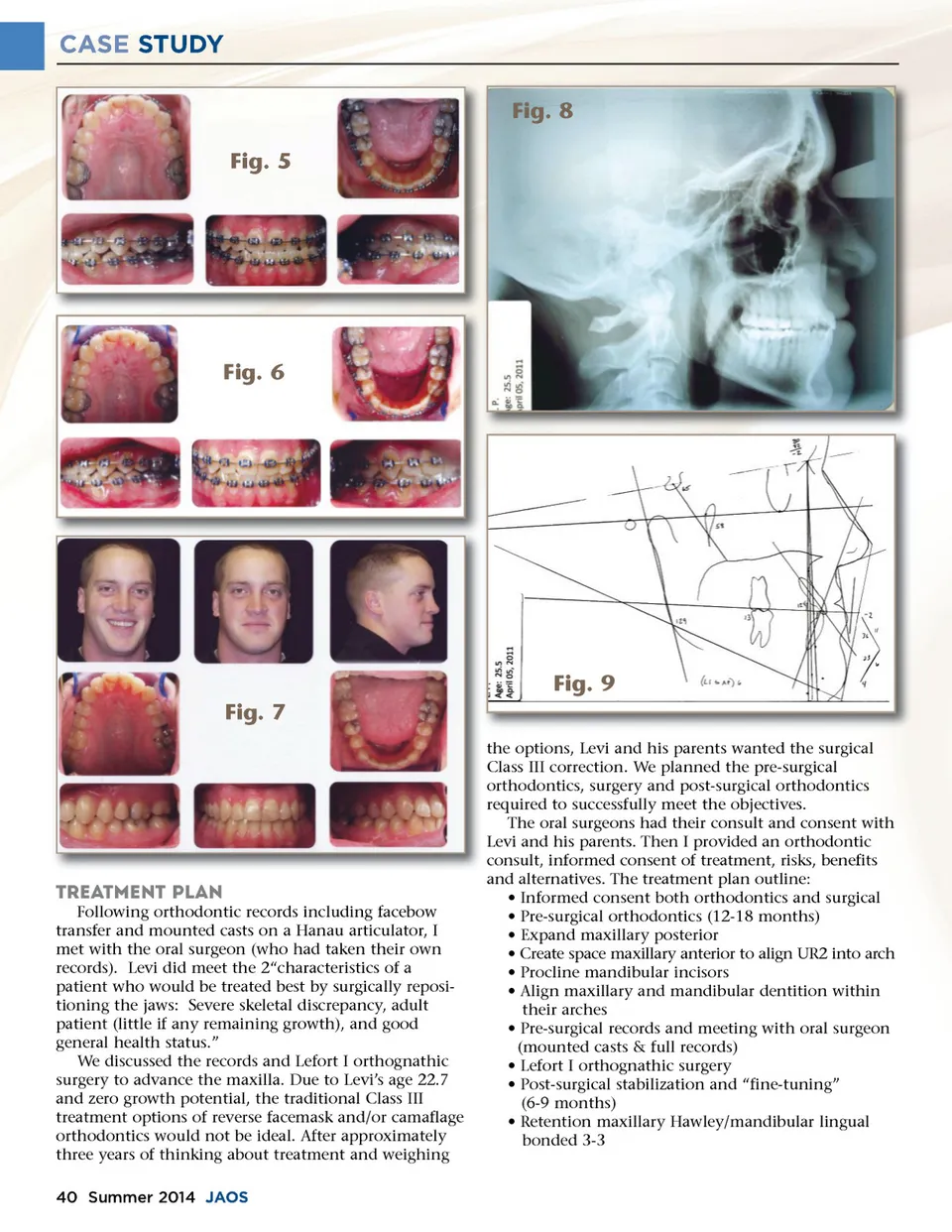
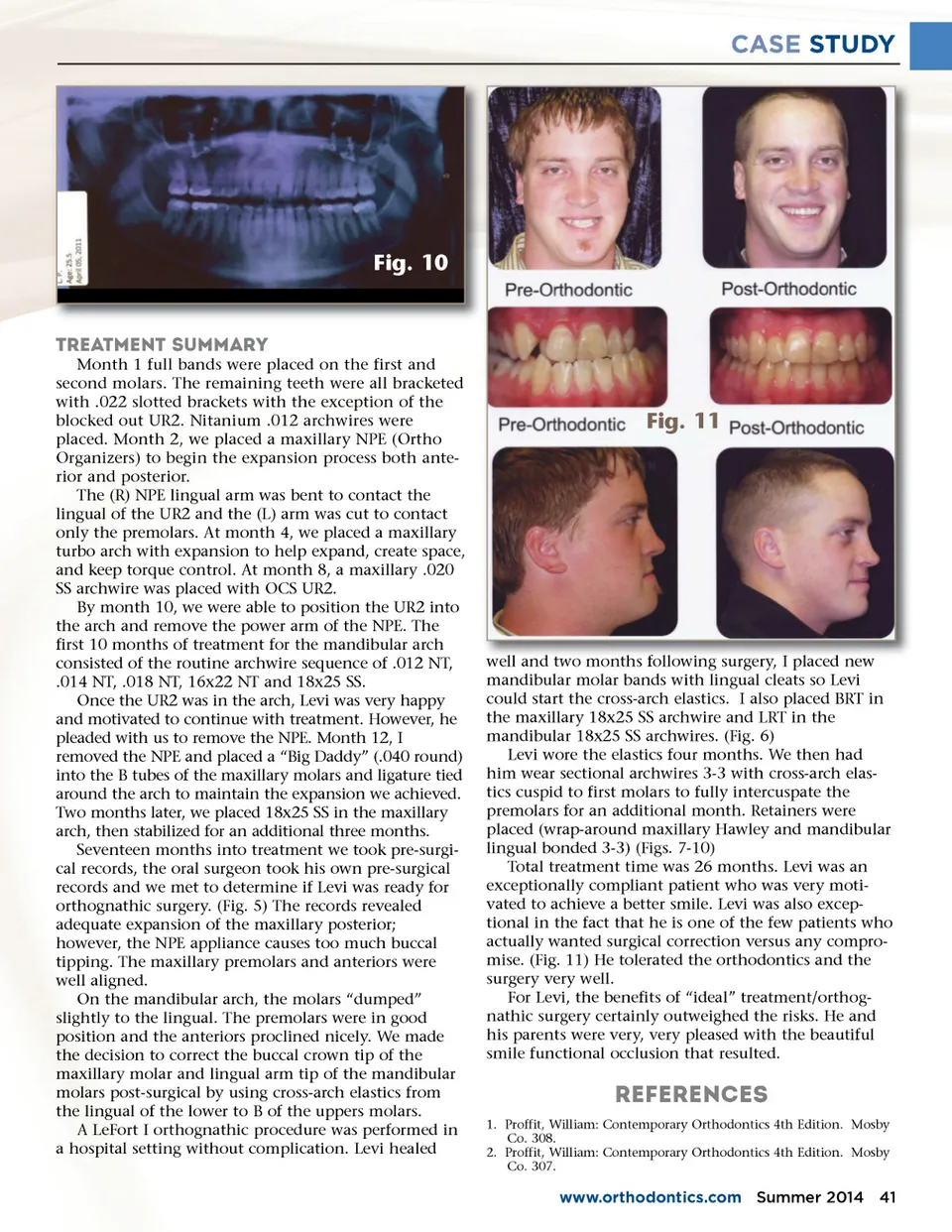
CASE STUDY Fig. 10 TREATMENT SUMMARY Month 1 full bands were placed on the first and second molars. The remaining teeth were all bracketed with .022 slotted brackets with the exception of the blocked out UR2. Nitanium .012 archwires were placed. Month 2, we placed a maxillary NPE (Ortho Organizers) to begin the expansion process both ante-rior and posterior. The (R) NPE lingual arm was bent to contact the lingual of the UR2 and the (L) arm was cut to contact only the premolars. At month 4, we placed a maxillary turbo arch with expansion to help expand, create space, and keep torque control. At month 8, a maxillary .020 SS archwire was placed with OCS UR2. By month 10, we were able to position the UR2 into the arch and remove the power arm of the NPE. The first 10 months of treatment for the mandibular arch consisted of the routine archwire sequence of .012 NT, .014 NT, .018 NT, 16x22 NT and 18x25 SS. Once the UR2 was in the arch, Levi was very happy and motivated to continue with treatment. However, he pleaded with us to remove the NPE. Month 12, I removed the NPE and placed a “Big Daddy” (.040 round) into the B tubes of the maxillary molars and ligature tied around the arch to maintain the expansion we achieved. Two months later, we placed 18x25 SS in the maxillary arch, then stabilized for an additional three months. Seventeen months into treatment we took pre-surgi-cal records, the oral surgeon took his own pre-surgical records and we met to determine if Levi was ready for orthognathic surgery. (Fig. 5) The records revealed adequate expansion of the maxillary posterior; however, the NPE appliance causes too much buccal tipping. The maxillary premolars and anteriors were well aligned. On the mandibular arch, the molars “dumped” slightly to the lingual. The premolars were in good position and the anteriors proclined nicely. We made the decision to correct the buccal crown tip of the maxillary molar and lingual arm tip of the mandibular molars post-surgical by using cross-arch elastics from the lingual of the lower to B of the uppers molars. A LeFort I orthognathic procedure was performed in a hospital setting without complication. Levi healed Fig. 11 well and two months following surgery surgery, I placed new mandibular molar bands with lingual cleats so Levi could start the cross-arch elastics. I also placed BRT in the maxillary 18x25 SS archwire and LRT in the mandibular 18x25 SS archwires. (Fig. 6) Levi wore the elastics four months. We then had him wear sectional archwires 3-3 with cross-arch elas-tics cuspid to first molars to fully intercuspate the premolars for an additional month. Retainers were placed (wrap-around maxillary Hawley and mandibular lingual bonded 3-3) (Figs. 7-10) Total treatment time was 26 months. Levi was an exceptionally compliant patient who was very moti-vated to achieve a better smile. Levi was also excep-tional in the fact that he is one of the few patients who actually wanted surgical correction versus any compro-mise. (Fig. 11) He tolerated the orthodontics and the surgery very well. For Levi, the benefits of “ideal” treatment/orthog-nathic surgery certainly outweighed the risks. He and his parents were very, very pleased with the beautiful smile functional occlusion that resulted. References 1. Proffit, William: Contemporary Orthodontics 4th Edition. Mosby Co. 308. 2. Proffit, William: Contemporary Orthodontics 4th Edition. Mosby Co. 307. www.orthodontics.com Summer 2014 41
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 41