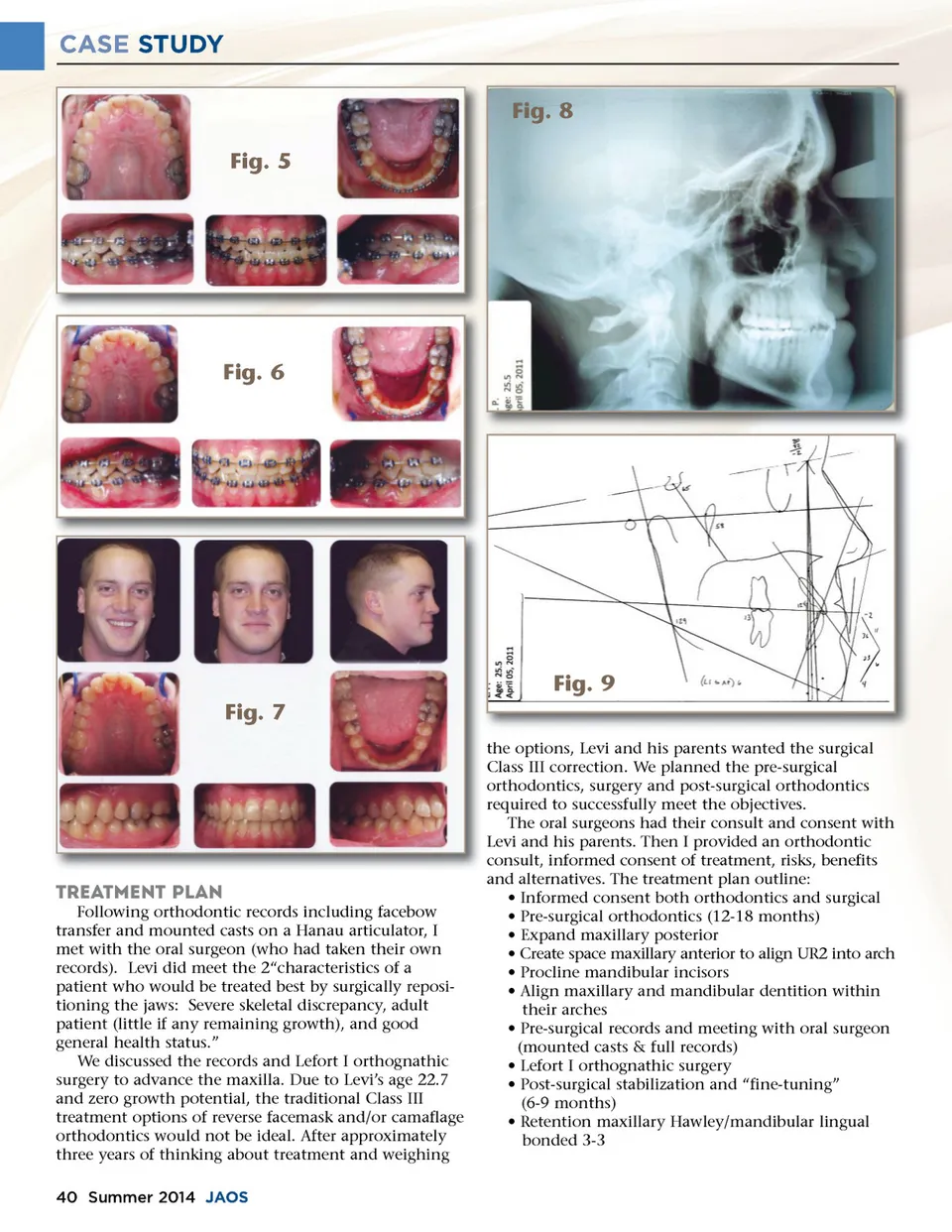
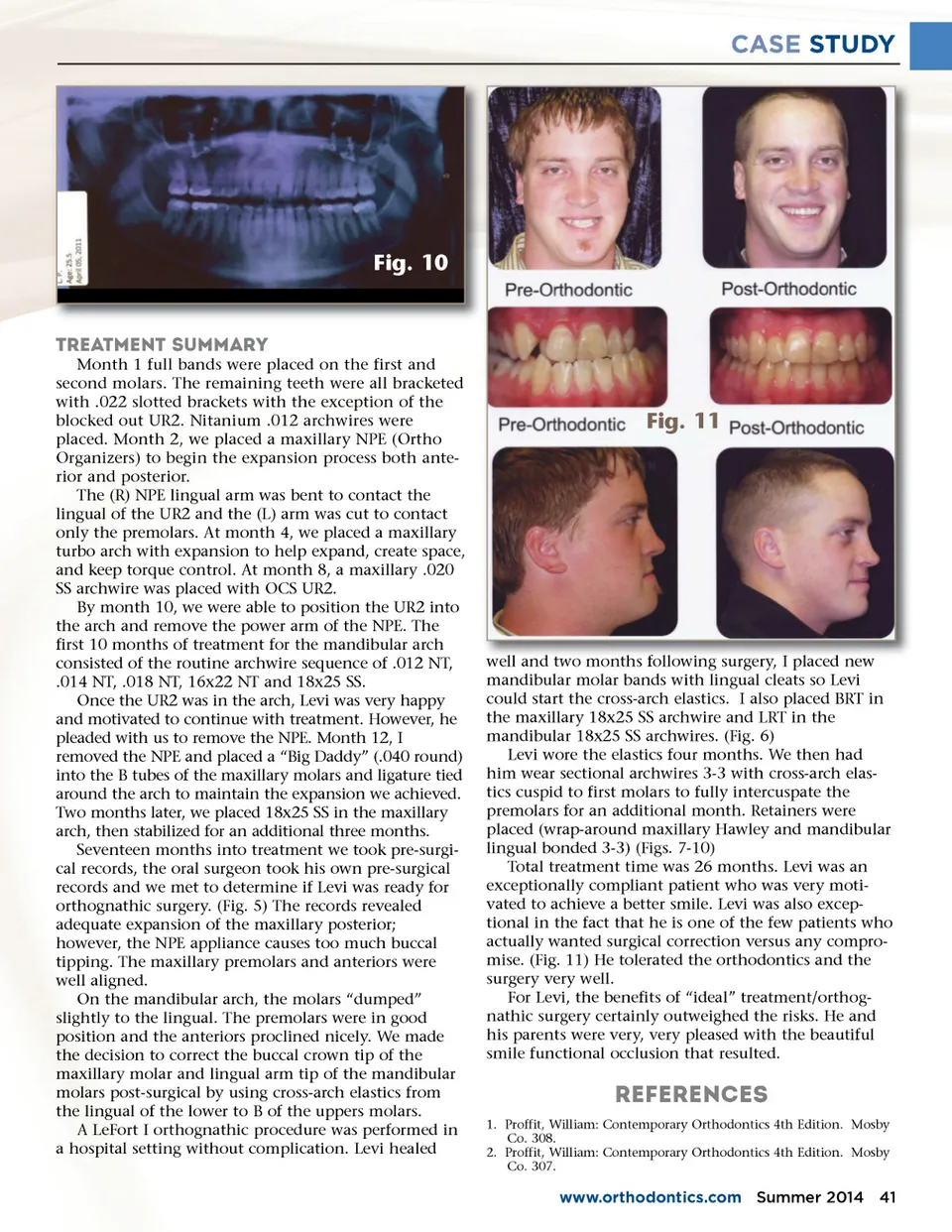
CASE STUDY Fig. 8 Fig. 5 Fig. 6 Fig. 9 Fig. 7 the options, Levi and his parents wanted the surgical Class III correction. We planned the pre-surgical orthodontics, surgery and post-surgical orthodontics required to successfully meet the objectives. The oral surgeons had their consult and consent with Levi and his parents. Then I provided an orthodontic consult, informed consent of treatment, risks, benefits and alternatives. The treatment plan outline: • Informed consent both orthodontics and surgical • Pre-surgical orthodontics (12-18 months) • Expand maxillary posterior • Create space maxillary anterior to align UR2 into arch • Procline mandibular incisors • Align maxillary and mandibular dentition within their arches • Pre-surgical records and meeting with oral surgeon (mounted casts & full records) • Lefort I orthognathic surgery • Post-surgical stabilization and “fine-tuning” (6-9 months) • Retention maxillary Hawley/mandibular lingual bonded 3-3 TREATMENT PLAN Following orthodontic records including facebow transfer and mounted casts on a Hanau articulator, I met with the oral surgeon (who had taken their own records). Levi did meet the 2“characteristics of a patient who would be treated best by surgically reposi-tioning the jaws: Severe skeletal discrepancy, adult patient (little if any remaining growth), and good general health status.” We discussed the records and Lefort I orthognathic surgery to advance the maxilla. Due to Levi’s age 22.7 and zero growth potential, the traditional Class III treatment options of reverse facemask and/or camaflage orthodontics would not be ideal. After approximately three years of thinking about treatment and weighing 40 Summer 2014 JAOS
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 40