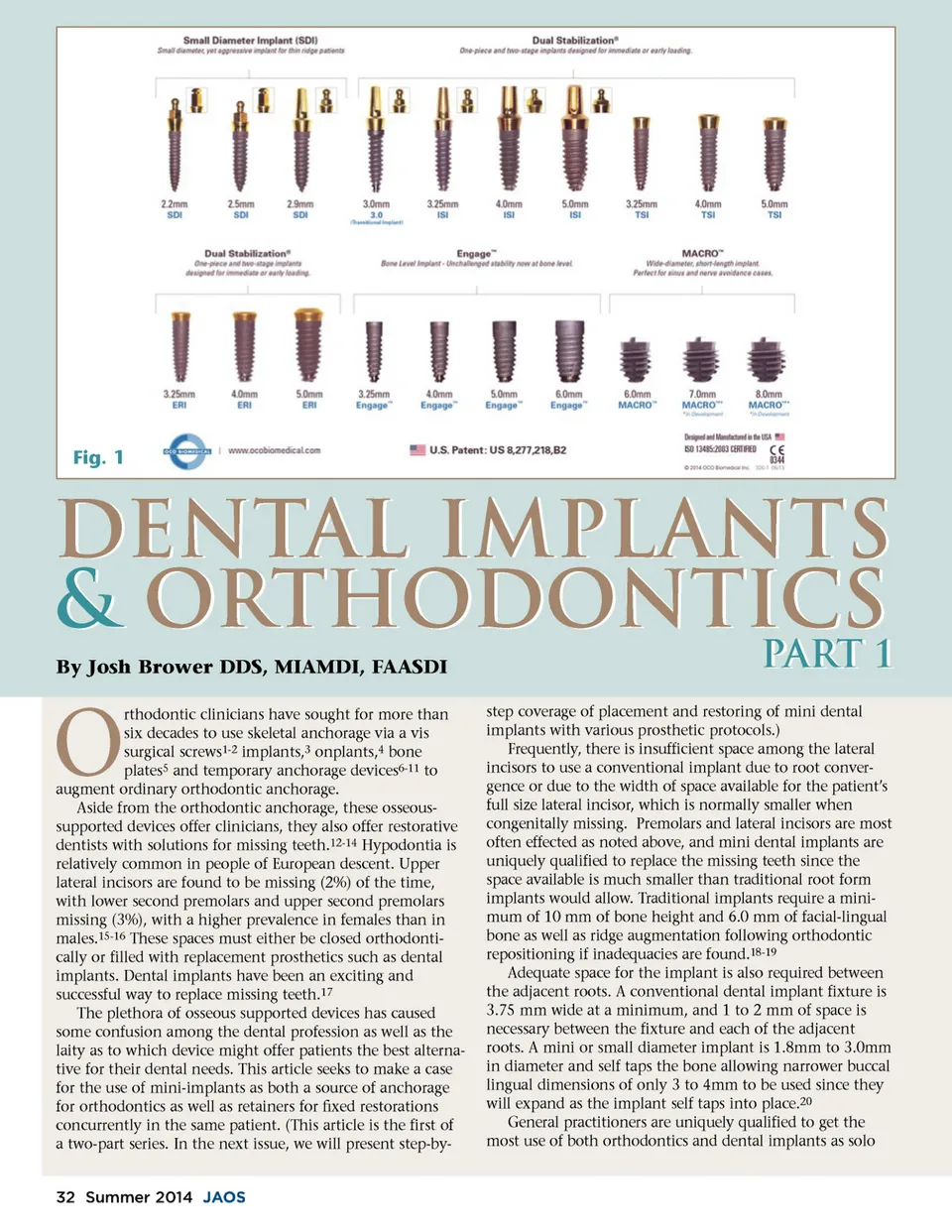
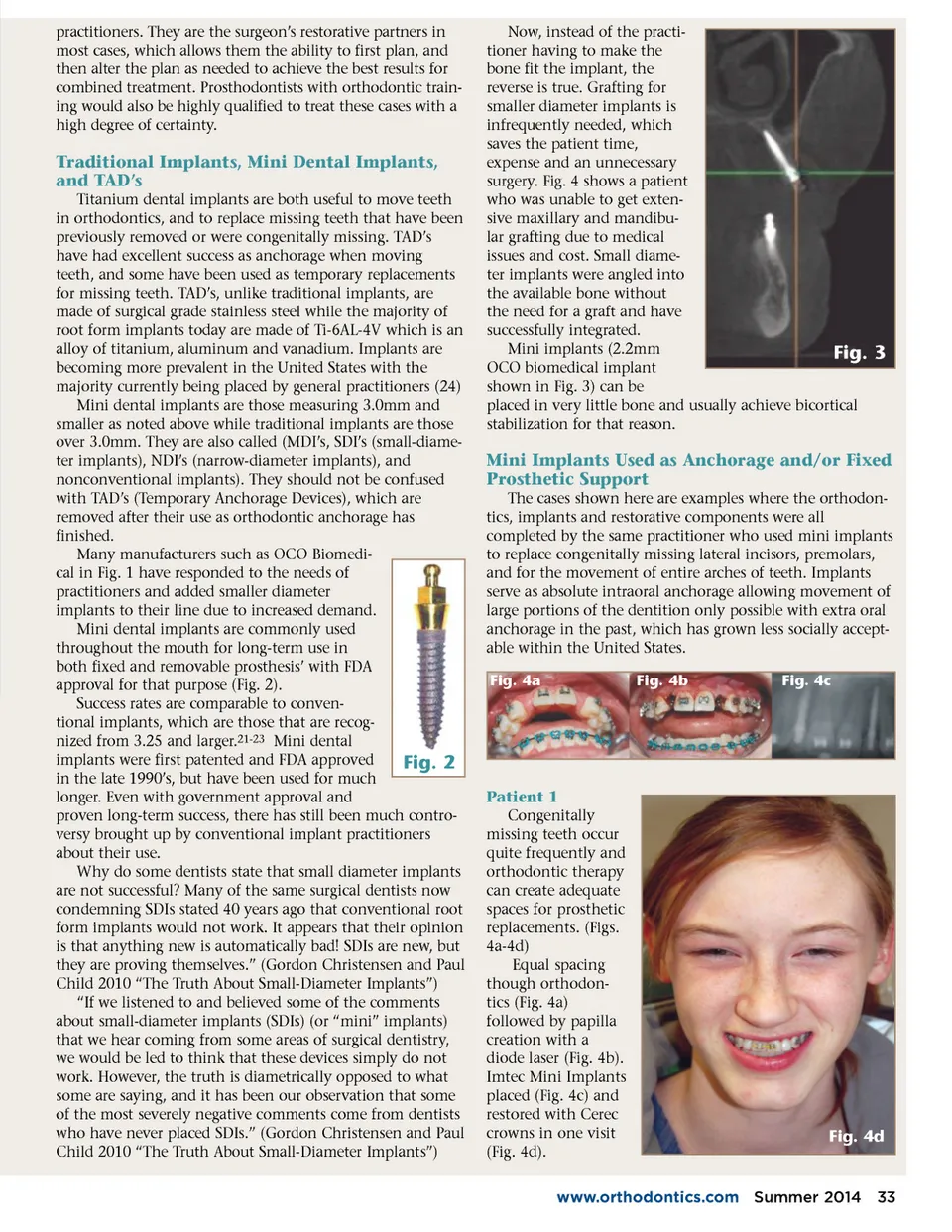
practitioners. They are the surgeon’s restorative partners in most cases, which allows them the ability to first plan, and then alter the plan as needed to achieve the best results for combined treatment. Prosthodontists with orthodontic train-ing would also be highly qualified to treat these cases with a high degree of certainty. Traditional Implants, Mini Dental Implants, and TAD’s Titanium dental implants are both useful to move teeth in orthodontics, and to replace missing teeth that have been previously removed or were congenitally missing. TAD’s have had excellent success as anchorage when moving teeth, and some have been used as temporary replacements for missing teeth. TAD’s, unlike traditional implants, are made of surgical grade stainless steel while the majority of root form implants today are made of Ti-6AL-4V which is an alloy of titanium, aluminum and vanadium. Implants are becoming more prevalent in the United States with the majority currently being placed by general practitioners (24) Mini dental implants are those measuring 3.0mm and smaller as noted above while traditional implants are those over 3.0mm. They are also called (MDI’s, SDI’s (small-diame-ter implants), NDI’s (narrow-diameter implants), and nonconventional implants). They should not be confused with TAD’s (Temporary Anchorage Devices), which are removed after their use as orthodontic anchorage has finished. Many manufacturers such as OCO Biomedi-cal in Fig. 1 have responded to the needs of practitioners and added smaller diameter implants to their line due to increased demand. Mini dental implants are commonly used throughout the mouth for long-term use in both fixed and removable prosthesis’ with FDA approval for that purpose (Fig. 2). Success rates are comparable to conven-tional implants, which are those that are recog-nized from 3.25 and larger. 21-23 Mini dental implants were first patented and FDA approved Fig. 2 in the late 1990’s, but have been used for much longer. Even with government approval and proven long-term success, there has still been much contro-versy brought up by conventional implant practitioners about their use. Why do some dentists state that small diameter implants are not successful? Many of the same surgical dentists now condemning SDIs stated 40 years ago that conventional root form implants would not work. It appears that their opinion is that anything new is automatically bad! SDIs are new, but they are proving themselves.” (Gordon Christensen and Paul Child 2010 “The Truth About Small-Diameter Implants”) “If we listened to and believed some of the comments about small-diameter implants (SDIs) (or “mini” implants) that we hear coming from some areas of surgical dentistry, we would be led to think that these devices simply do not work. However, the truth is diametrically opposed to what some are saying, and it has been our observation that some of the most severely negative comments come from dentists who have never placed SDIs.” (Gordon Christensen and Paul Child 2010 “The Truth About Small-Diameter Implants”) Now, instead of the practi-tioner having to make the bone fit the implant, the reverse is true. Grafting for smaller diameter implants is infrequently needed, which saves the patient time, expense and an unnecessary surgery. Fig. 4 shows a patient who was unable to get exten-sive maxillary and mandibu-lar grafting due to medical issues and cost. Small diame-ter implants were angled into the available bone without the need for a graft and have successfully integrated. Mini implants (2.2mm Fig. 3 OCO biomedical implant shown in Fig. 3) can be placed in very little bone and usually achieve bicortical stabilization for that reason. Mini Implants Used as Anchorage and/or Fixed Prosthetic Support The cases shown here are examples where the orthodon-tics, implants and restorative components were all completed by the same practitioner who used mini implants to replace congenitally missing lateral incisors, premolars, and for the movement of entire arches of teeth. Implants serve as absolute intraoral anchorage allowing movement of large portions of the dentition only possible with extra oral anchorage in the past, which has grown less socially accept-able within the United States. Fig. 4a Fig. 4b Fig. 4c Patient 1 Congenitally missing teeth occur quite frequently and orthodontic therapy can create adequate spaces for prosthetic replacements. (Figs. 4a-4d) Equal spacing though orthodon-tics (Fig. 4a) followed by papilla creation with a diode laser (Fig. 4b). Imtec Mini Implants placed (Fig. 4c) and restored with Cerec crowns in one visit (Fig. 4d). Fig. 4d www.orthodontics.com Summer 2014 33
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 33