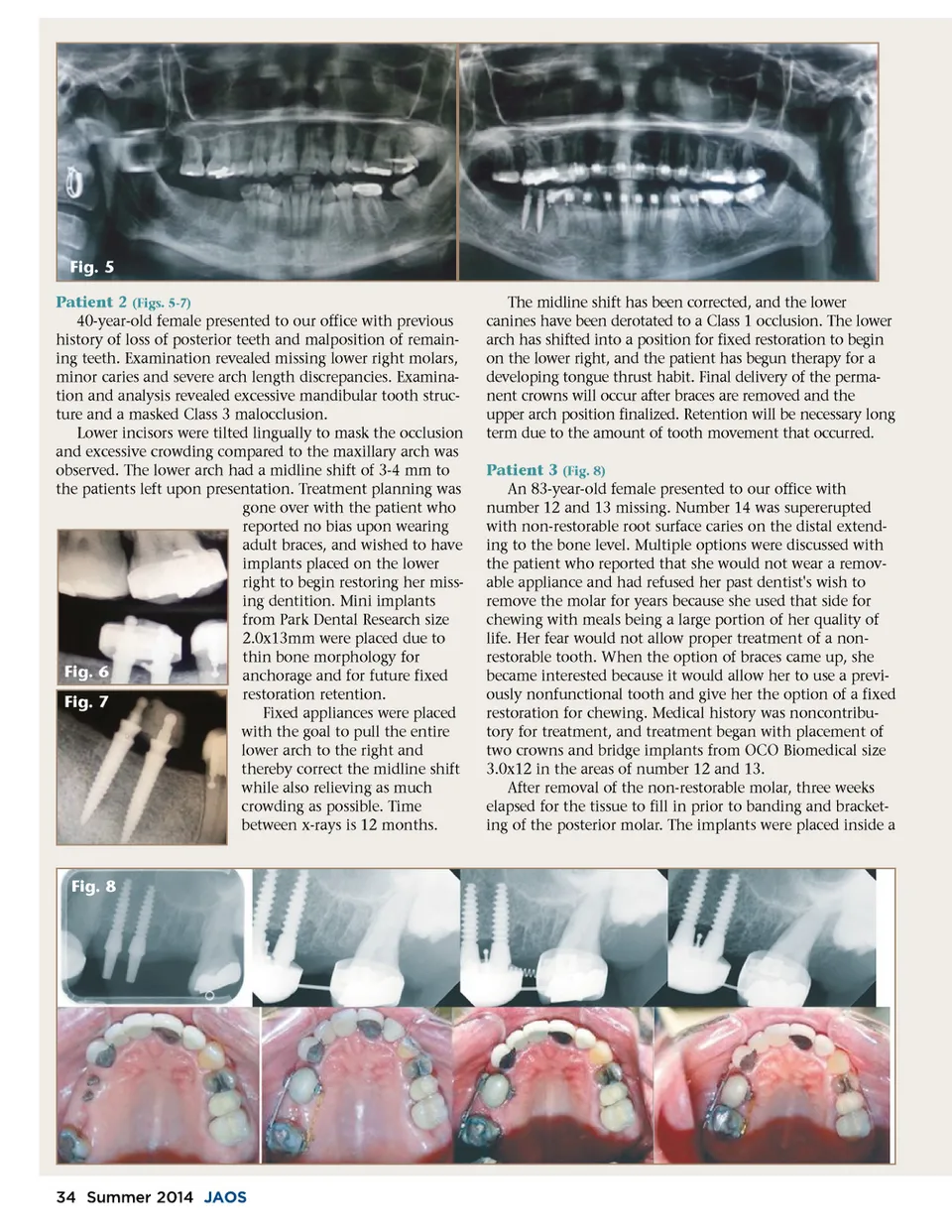
Fig. 5 Patient 2 (Figs. 5-7) 40-year-old female presented to our office with previous history of loss of posterior teeth and malposition of remain-ing teeth. Examination revealed missing lower right molars, minor caries and severe arch length discrepancies. Examina-tion and analysis revealed excessive mandibular tooth struc-ture and a masked Class 3 malocclusion. Lower incisors were tilted lingually to mask the occlusion and excessive crowding compared to the maxillary arch was observed. The lower arch had a midline shift of 3-4 mm to the patients left upon presentation. Treatment planning was gone over with the patient who reported no bias upon wearing adult braces, and wished to have implants placed on the lower right to begin restoring her miss-ing dentition. Mini implants from Park Dental Research size 2.0x13mm were placed due to thin bone morphology for Fig. 6 anchorage and for future fixed restoration retention. Fig. 7 Fixed appliances were placed with the goal to pull the entire lower arch to the right and thereby correct the midline shift while also relieving as much crowding as possible. Time between x-rays is 12 months. The midline shift has been corrected, and the lower canines have been derotated to a Class 1 occlusion. The lower arch has shifted into a position for fixed restoration to begin on the lower right, and the patient has begun therapy for a developing tongue thrust habit. Final delivery of the perma-nent crowns will occur after braces are removed and the upper arch position finalized. Retention will be necessary long term due to the amount of tooth movement that occurred. Patient 3 (Fig. 8) An 83-year-old female presented to our office with number 12 and 13 missing. Number 14 was supererupted with non-restorable root surface caries on the distal extend-ing to the bone level. Multiple options were discussed with the patient who reported that she would not wear a remov-able appliance and had refused her past dentist's wish to remove the molar for years because she used that side for chewing with meals being a large portion of her quality of life. Her fear would not allow proper treatment of a non-restorable tooth. When the option of braces came up, she became interested because it would allow her to use a previ-ously nonfunctional tooth and give her the option of a fixed restoration for chewing. Medical history was noncontribu-tory for treatment, and treatment began with placement of two crowns and bridge implants from OCO Biomedical size 3.0x12 in the areas of number 12 and 13. After removal of the non-restorable molar, three weeks elapsed for the tissue to fill in prior to banding and bracket-ing of the posterior molar. The implants were placed inside a Fig. 8 34 Summer 2014 JAOS
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 34