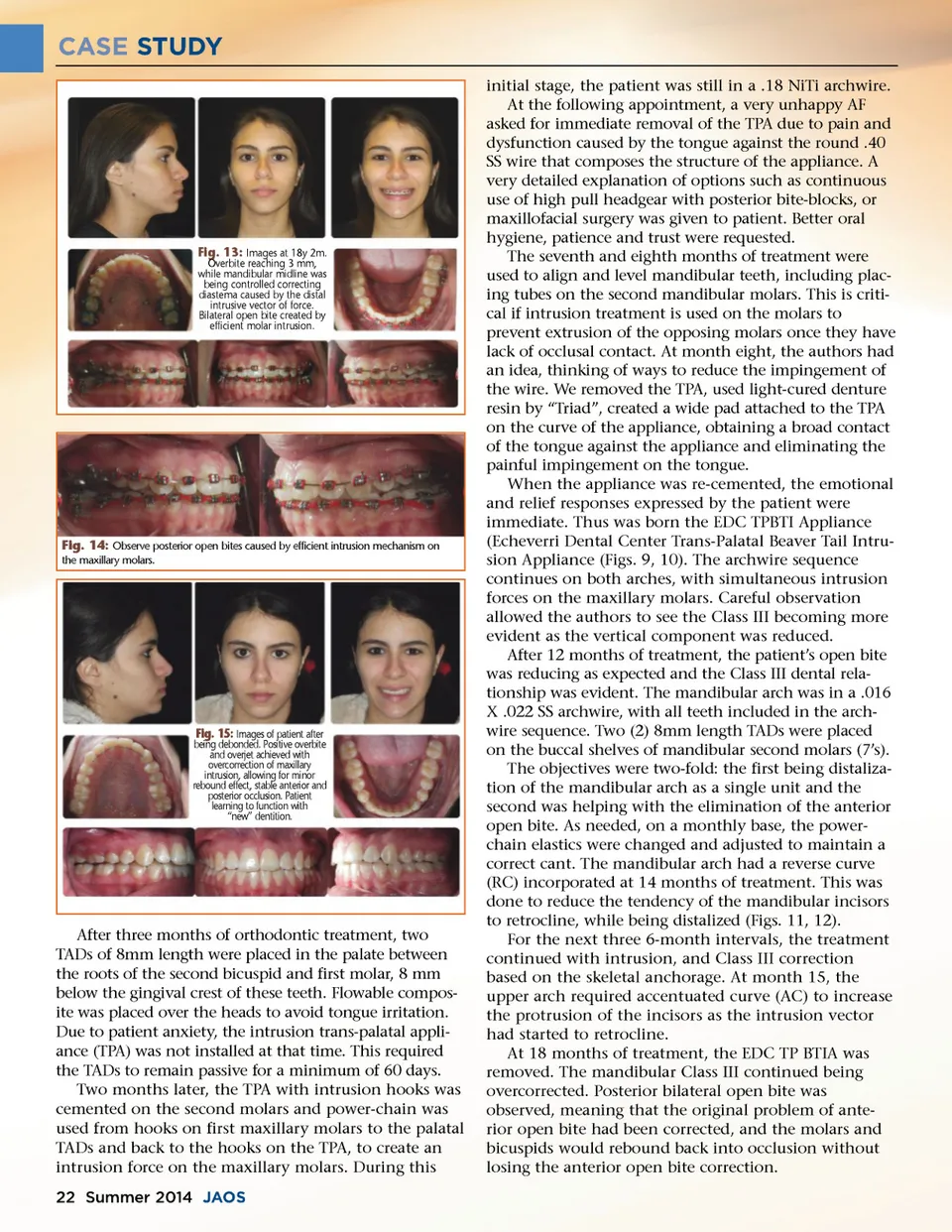
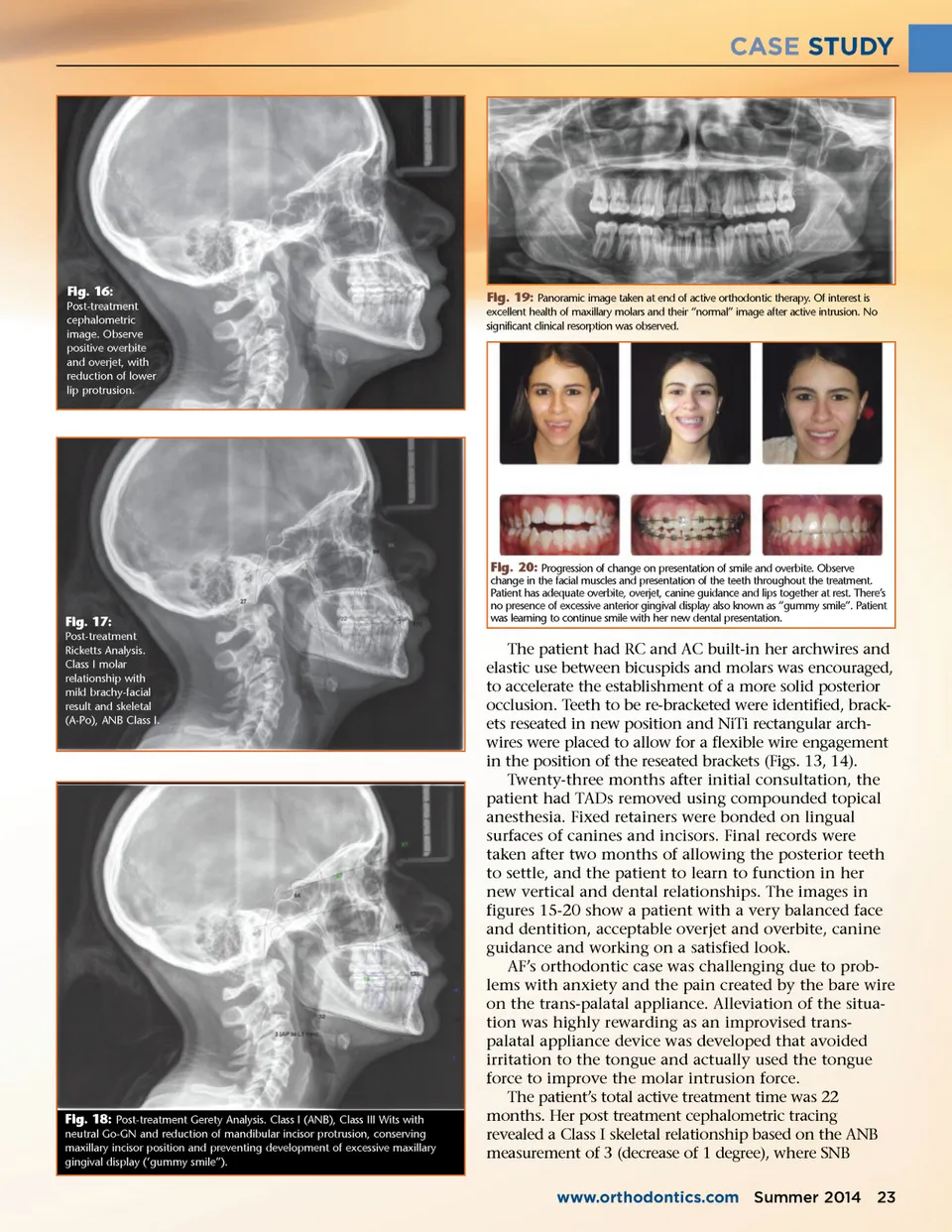
CASE STUDY Fig. 16: Post-treatment cephalometric image. Observe positive overbite and overjet, with reduction of lower lip protrusion. Fig. 19: Panoramic image taken at end of active orthodontic therapy. Of interest is excellent health of maxillary molars and their “normal” image after active intrusion. No significant clinical resorption was observed. Fig. 17: Post-treatment Ricketts Analysis. Class I molar relationship with mild brachy-facial result and skeletal (A-Po), ANB Class I. Fig. 20: Progression of change on presentation of smile and overbite. Observe change in the facial muscles and presentation of the teeth throughout the treatment. Patient has adequate overbite, overjet, canine guidance and lips together at rest. There’s no presence of excessive anterior gingival display also known as “gummy smile”. Patient was learning to continue smile with her new dental presentation. Fig. 18: Post-treatment Gerety Analysis. Class I (ANB), Class III Wits with neutral Go-GN and reduction of mandibular incisor protrusion, conserving maxillary incisor position and preventing development of excessive maxillary gingival display (‘gummy smile”). The patient had RC and AC built-in her archwires and elastic use between bicuspids and molars was encouraged, to accelerate the establishment of a more solid posterior occlusion. Teeth to be re-bracketed were identified, brack-ets reseated in new position and NiTi rectangular arch-wires were placed to allow for a flexible wire engagement in the position of the reseated brackets (Figs. 13, 14). Twenty-three months after initial consultation, the patient had TADs removed using compounded topical anesthesia. Fixed retainers were bonded on lingual surfaces of canines and incisors. Final records were taken after two months of allowing the posterior teeth to settle, and the patient to learn to function in her new vertical and dental relationships. The images in figures 15-20 show a patient with a very balanced face and dentition, acceptable overjet and overbite, canine guidance and working on a satisfied look. AF’s orthodontic case was challenging due to prob-lems with anxiety and the pain created by the bare wire on the trans-palatal appliance. Alleviation of the situa-tion was highly rewarding as an improvised trans-palatal appliance device was developed that avoided irritation to the tongue and actually used the tongue force to improve the molar intrusion force. The patient’s total active treatment time was 22 months. Her post treatment cephalometric tracing revealed a Class I skeletal relationship based on the ANB measurement of 3 (decrease of 1 degree), where SNB www.orthodontics.com Summer 2014 23
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 23