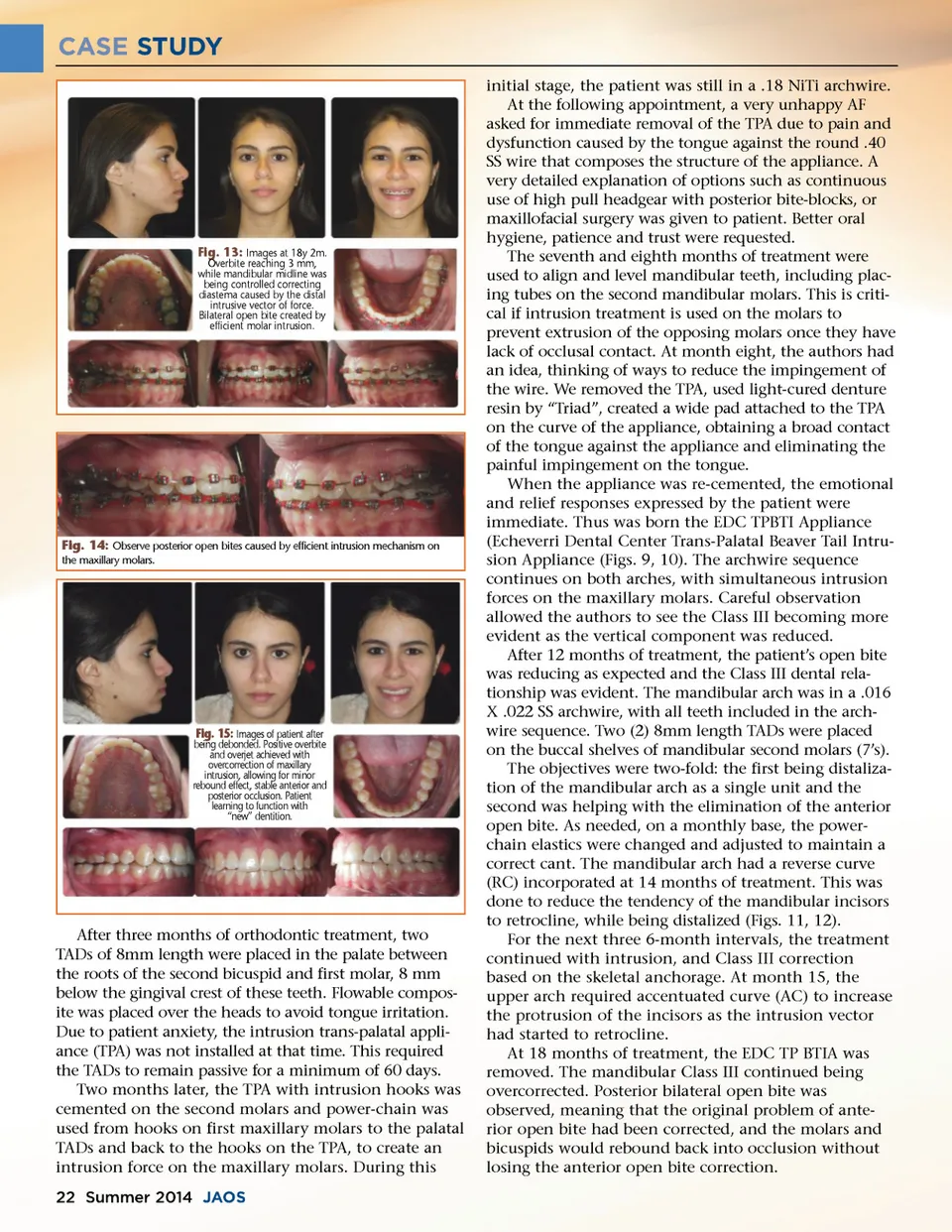
CASE STUDY initial stage, the patient was still in a .18 NiTi archwire. At the following appointment, a very unhappy AF asked for immediate removal of the TPA due to pain and dysfunction caused by the tongue against the round .40 SS wire that composes the structure of the appliance. A very detailed explanation of options such as continuous use of high pull headgear with posterior bite-blocks, or maxillofacial surgery was given to patient. Better oral hygiene, patience and trust were requested. The seventh and eighth months of treatment were used to align and level mandibular teeth, including plac-ing tubes on the second mandibular molars. This is criti-cal if intrusion treatment is used on the molars to prevent extrusion of the opposing molars once they have lack of occlusal contact. At month eight, the authors had an idea, thinking of ways to reduce the impingement of the wire. We removed the TPA, used light-cured denture resin by “Triad”, created a wide pad attached to the TPA on the curve of the appliance, obtaining a broad contact of the tongue against the appliance and eliminating the painful impingement on the tongue. When the appliance was re-cemented, the emotional and relief responses expressed by the patient were immediate. Thus was born the EDC TPBTI Appliance (Echeverri Dental Center Trans-Palatal Beaver Tail Intru-sion Appliance (Figs. 9, 10). The archwire sequence continues on both arches, with simultaneous intrusion forces on the maxillary molars. Careful observation allowed the authors to see the Class III becoming more evident as the vertical component was reduced. After 12 months of treatment, the patient’s open bite was reducing as expected and the Class III dental rela-tionship was evident. The mandibular arch was in a .016 X .022 SS archwire, with all teeth included in the arch-wire sequence. Two (2) 8mm length TADs were placed on the buccal shelves of mandibular second molars (7’s). The objectives were two-fold: the first being distaliza-tion of the mandibular arch as a single unit and the second was helping with the elimination of the anterior open bite. As needed, on a monthly base, the power-chain elastics were changed and adjusted to maintain a correct cant. The mandibular arch had a reverse curve (RC) incorporated at 14 months of treatment. This was done to reduce the tendency of the mandibular incisors to retrocline, while being distalized (Figs. 11, 12). For the next three 6-month intervals, the treatment continued with intrusion, and Class III correction based on the skeletal anchorage. At month 15, the upper arch required accentuated curve (AC) to increase the protrusion of the incisors as the intrusion vector had started to retrocline. At 18 months of treatment, the EDC TP BTIA was removed. The mandibular Class III continued being overcorrected. Posterior bilateral open bite was observed, meaning that the original problem of ante-rior open bite had been corrected, and the molars and bicuspids would rebound back into occlusion without losing the anterior open bite correction. Fig. 13: Images at 18y 2m. Overbite reaching 3 mm, while mandibular midline was being controlled correcting diastema caused by the distal intrusive vector of force. Bilateral open bite created by efficient molar intrusion. Fig. 14: Observe posterior open bites caused by efficient intrusion mechanism on the maxillary molars. Fig. 15: Images of patient after being debonded. Positive overbite and overjet achieved with overcorrection of maxillary intrusion, allowing for minor rebound effect, stable anterior and posterior occlusion. Patient learning to function with “new” dentition. After three months of orthodontic treatment, two TADs of 8mm length were placed in the palate between the roots of the second bicuspid and first molar, 8 mm below the gingival crest of these teeth. Flowable compos-ite was placed over the heads to avoid tongue irritation. Due to patient anxiety, the intrusion trans-palatal appli-ance (TPA) was not installed at that time. This required the TADs to remain passive for a minimum of 60 days. Two months later, the TPA with intrusion hooks was cemented on the second molars and power-chain was used from hooks on first maxillary molars to the palatal TADs and back to the hooks on the TPA, to create an intrusion force on the maxillary molars. During this 22 Summer 2014 JAOS
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 22