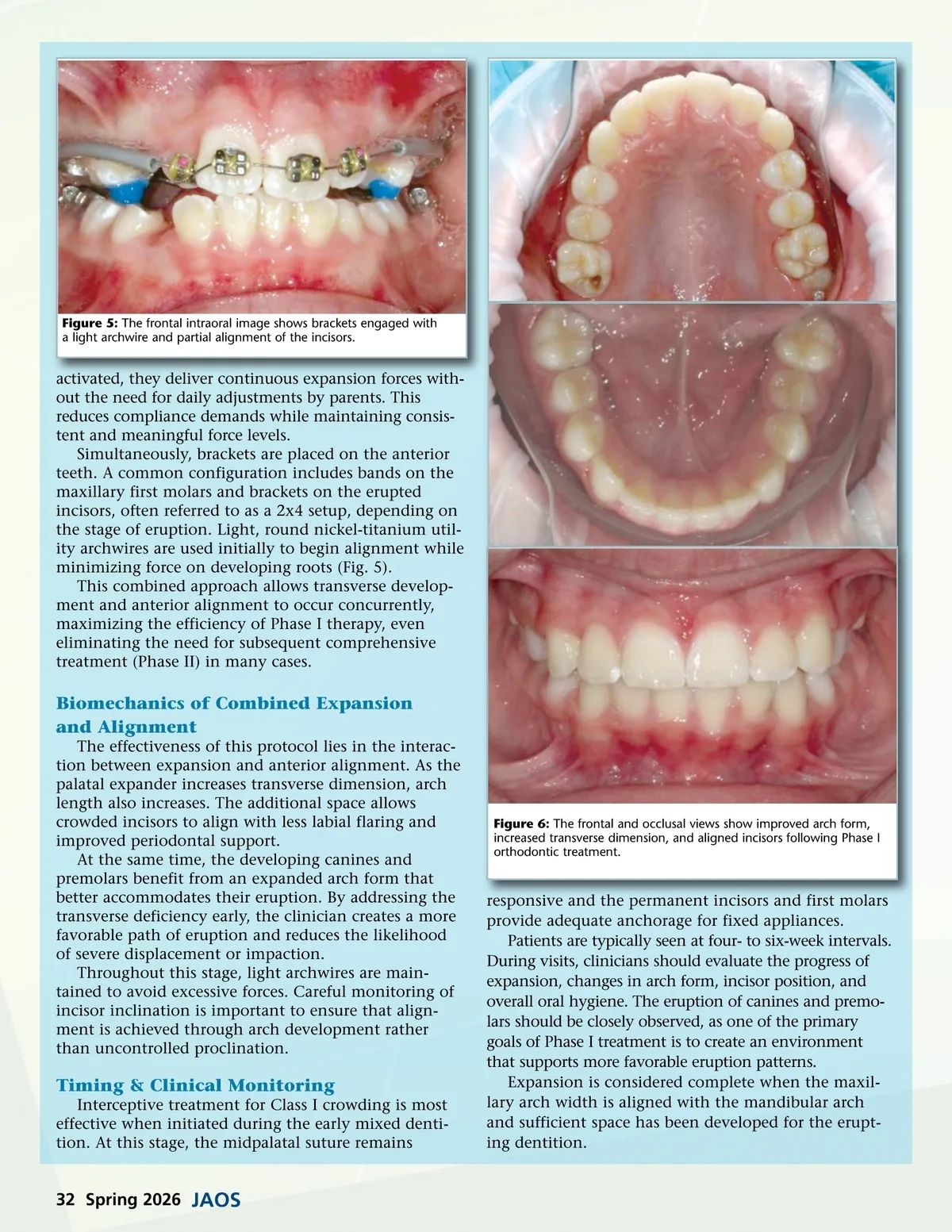
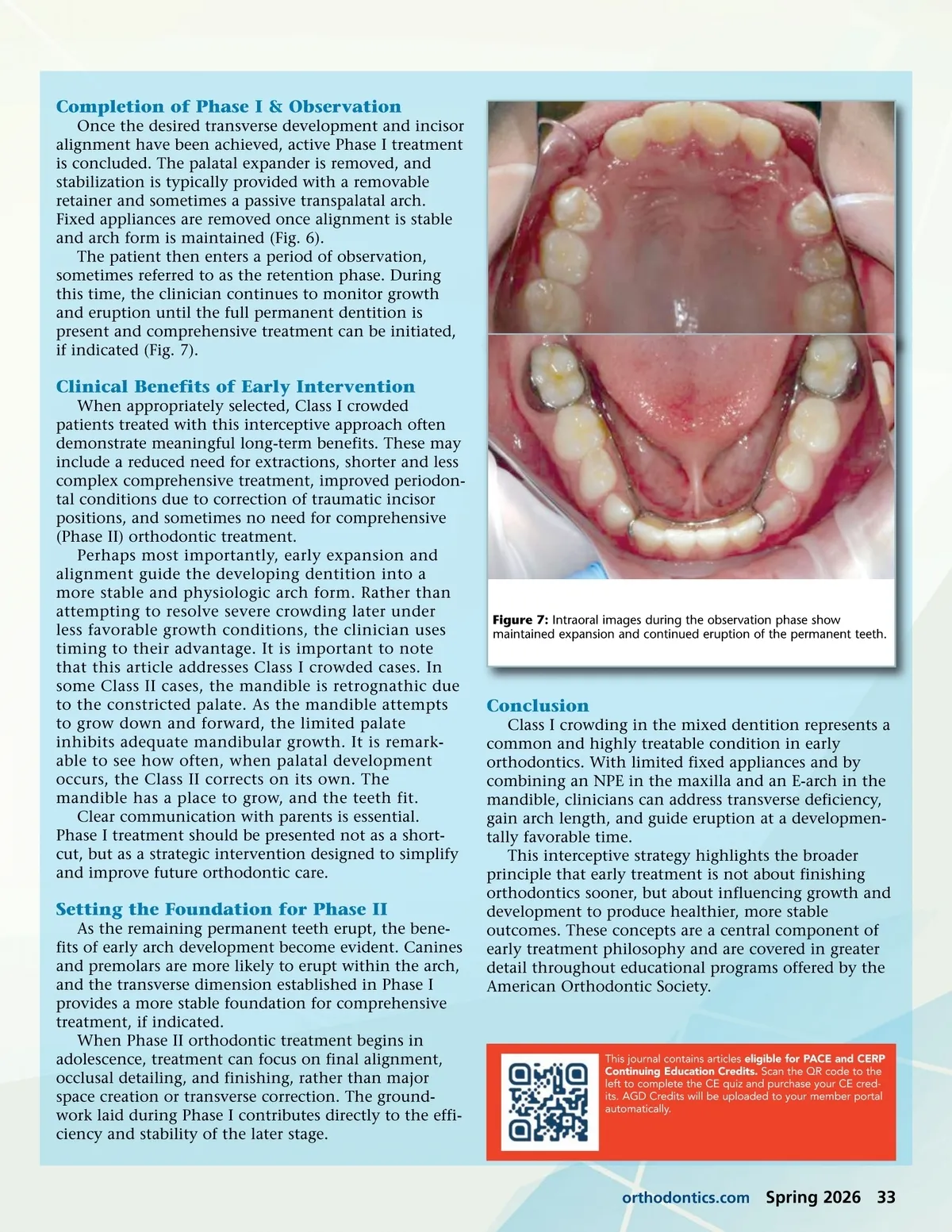
Figure 5: The frontal intraoral image shows brackets engaged with a light archwire and partial alignment of the incisors. activated, they deliver continuous expansion forces with-out the need for daily adjustments by parents. This reduces compliance demands while maintaining consis-tent and meaningful force levels. Simultaneously, brackets are placed on the anterior teeth. A common configuration includes bands on the maxillary first molars and brackets on the erupted incisors, often referred to as a 2x4 setup, depending on the stage of eruption. Light, round nickel-titanium util-ity archwires are used initially to begin alignment while minimizing force on developing roots (Fig. 5). This combined approach allows transverse develop-ment and anterior alignment to occur concurrently, maximizing the efficiency of Phase I therapy, even eliminating the need for subsequent comprehensive treatment (Phase II) in many cases. Biomechanics of Combined Expansion and Alignment The effectiveness of this protocol lies in the interac-tion between expansion and anterior alignment. As the palatal expander increases transverse dimension, arch length also increases. The additional space allows crowded incisors to align with less labial flaring and improved periodontal support. At the same time, the developing canines and premolars benefit from an expanded arch form that better accommodates their eruption. By addressing the transverse deficiency early, the clinician creates a more favorable path of eruption and reduces the likelihood of severe displacement or impaction. Throughout this stage, light archwires are main-tained to avoid excessive forces. Careful monitoring of incisor inclination is important to ensure that align-ment is achieved through arch development rather than uncontrolled proclination. Figure 6: The frontal and occlusal views show improved arch form, increased transverse dimension, and aligned incisors following Phase I orthodontic treatment. Timing & Clinical Monitoring Interceptive treatment for Class I crowding is most effective when initiated during the early mixed denti-tion. At this stage, the midpalatal suture remains responsive and the permanent incisors and first molars provide adequate anchorage for fixed appliances. Patients are typically seen at four-to six-week intervals. During visits, clinicians should evaluate the progress of expansion, changes in arch form, incisor position, and overall oral hygiene. The eruption of canines and premo-lars should be closely observed, as one of the primary goals of Phase I treatment is to create an environment that supports more favorable eruption patterns. Expansion is considered complete when the maxil-lary arch width is aligned with the mandibular arch and sufficient space has been developed for the erupt-ing dentition. 32 Spring 2026 JAOS
Journal of the American Orthodontic Society Spring 2026: Page 32