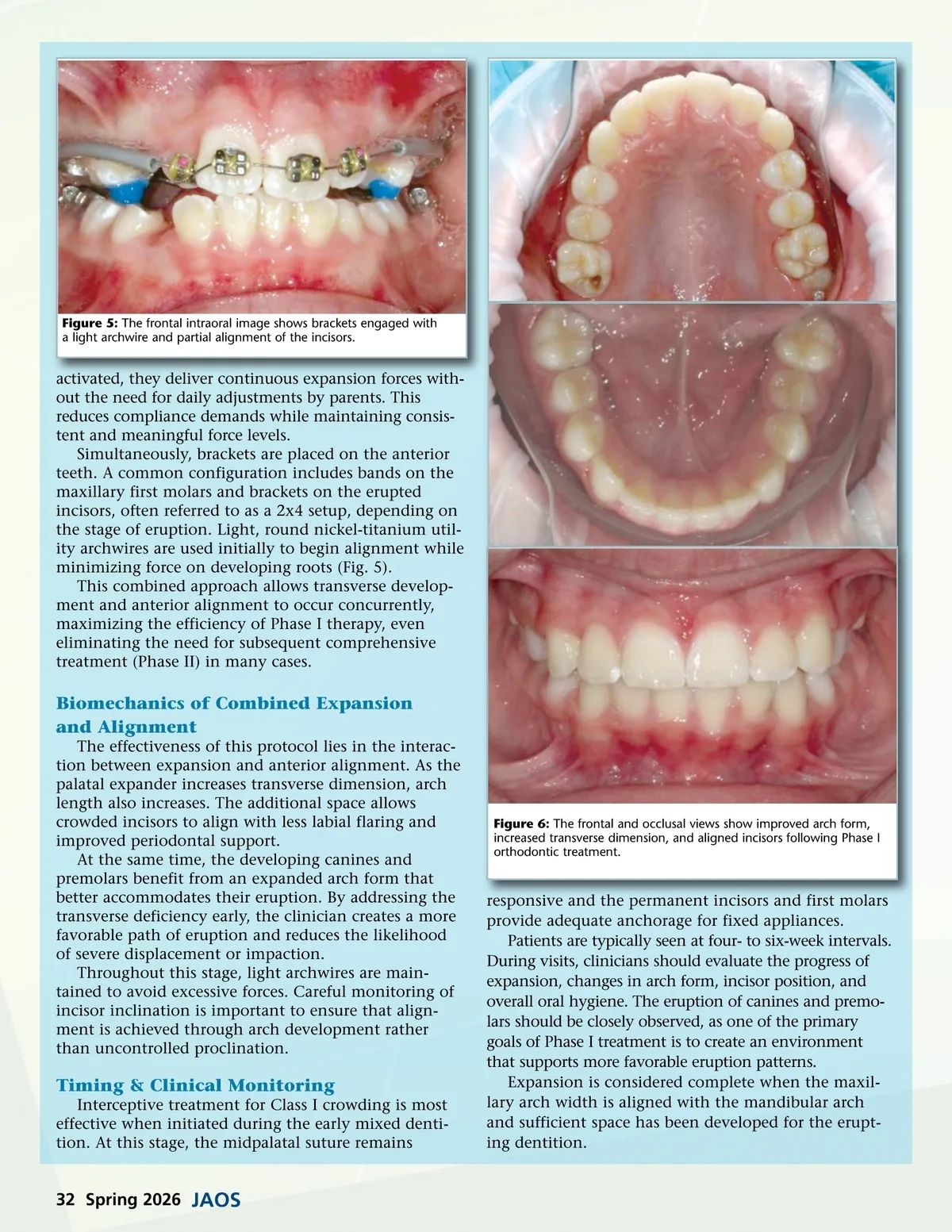
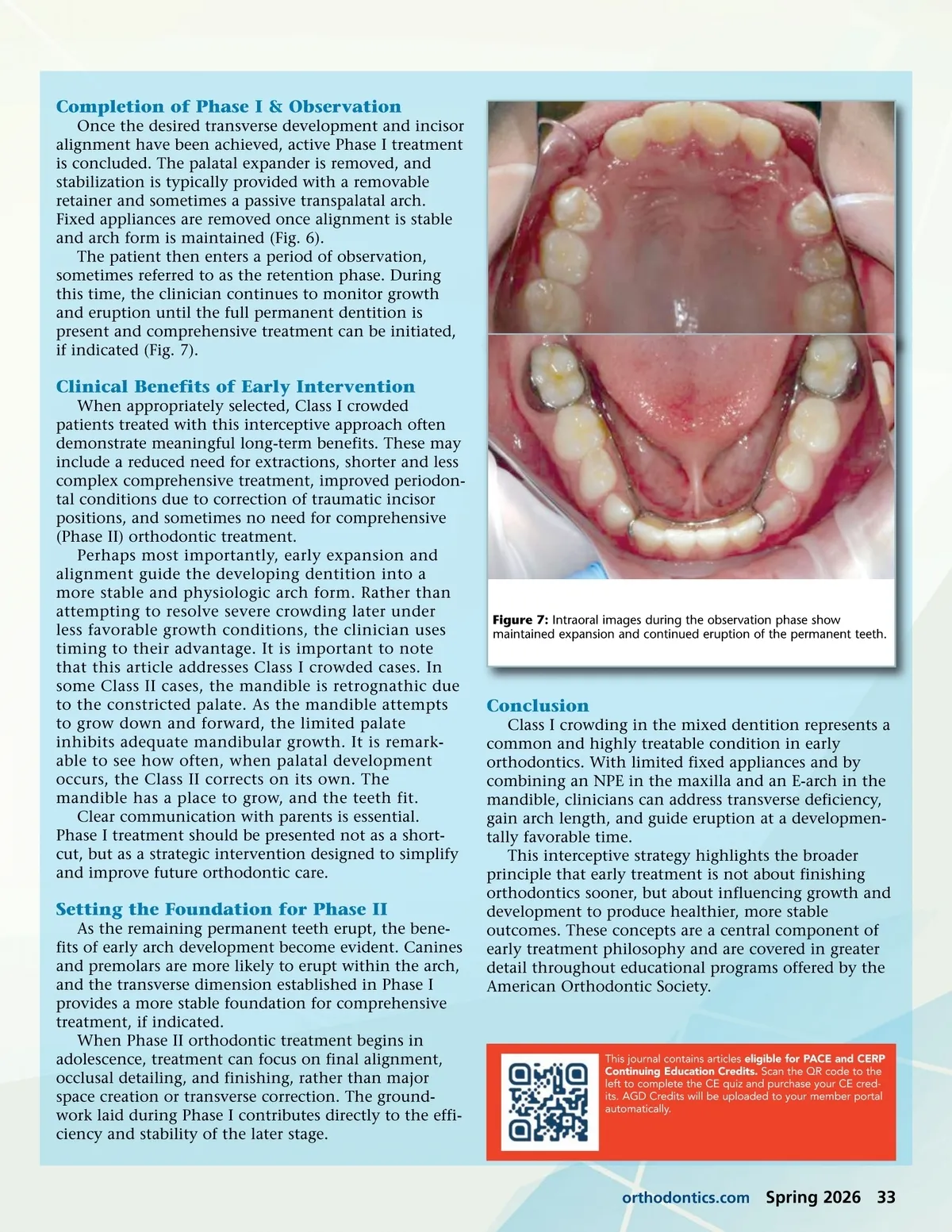
Completion of Phase I & Observation Once the desired transverse development and incisor alignment have been achieved, active Phase I treatment is concluded. The palatal expander is removed, and stabilization is typically provided with a removable retainer and sometimes a passive transpalatal arch. Fixed appliances are removed once alignment is stable and arch form is maintained (Fig. 6). The patient then enters a period of observation, sometimes referred to as the retention phase. During this time, the clinician continues to monitor growth and eruption until the full permanent dentition is present and comprehensive treatment can be initiated, if indicated (Fig. 7). Clinical Benefits of Early Intervention When appropriately selected, Class I crowded patients treated with this interceptive approach often demonstrate meaningful long-term benefits. These may include a reduced need for extractions, shorter and less complex comprehensive treatment, improved periodon-tal conditions due to correction of traumatic incisor positions, and sometimes no need for comprehensive (Phase II) orthodontic treatment. Perhaps most importantly, early expansion and alignment guide the developing dentition into a more stable and physiologic arch form. Rather than attempting to resolve severe crowding later under less favorable growth conditions, the clinician uses timing to their advantage. It is important to note that this article addresses Class I crowded cases. In some Class II cases, the mandible is retrognathic due to the constricted palate. As the mandible attempts to grow down and forward, the limited palate inhibits adequate mandibular growth. It is remark-able to see how often, when palatal development occurs, the Class II corrects on its own. The mandible has a place to grow, and the teeth fit. Clear communication with parents is essential. Phase I treatment should be presented not as a short-cut, but as a strategic intervention designed to simplify and improve future orthodontic care. Figure 7: Intraoral images during the observation phase show maintained expansion and continued eruption of the permanent teeth. Conclusion Class I crowding in the mixed dentition represents a common and highly treatable condition in early orthodontics. With limited fixed appliances and by combining an NPE in the maxilla and an E-arch in the mandible, clinicians can address transverse deficiency, gain arch length, and guide eruption at a developmen-tally favorable time. This interceptive strategy highlights the broader principle that early treatment is not about finishing orthodontics sooner, but about influencing growth and development to produce healthier, more stable outcomes. These concepts are a central component of early treatment philosophy and are covered in greater detail throughout educational programs offered by the American Orthodontic Society. Setting the Foundation for Phase II As the remaining permanent teeth erupt, the bene-fits of early arch development become evident. Canines and premolars are more likely to erupt within the arch, and the transverse dimension established in Phase I provides a more stable foundation for comprehensive treatment, if indicated. When Phase II orthodontic treatment begins in adolescence, treatment can focus on final alignment, occlusal detailing, and finishing, rather than major space creation or transverse correction. The ground-work laid during Phase I contributes directly to the effi-ciency and stability of the later stage. This journal contains articles eligible for PACE and CERP Continuing Education Credits. Scan the QR code to the left to complete the CE quiz and purchase your CE cred-its. AGD Credits will be uploaded to your member portal automatically. orthodontics.com Spring 2026 33
Journal of the American Orthodontic Society Spring 2026: Page 33