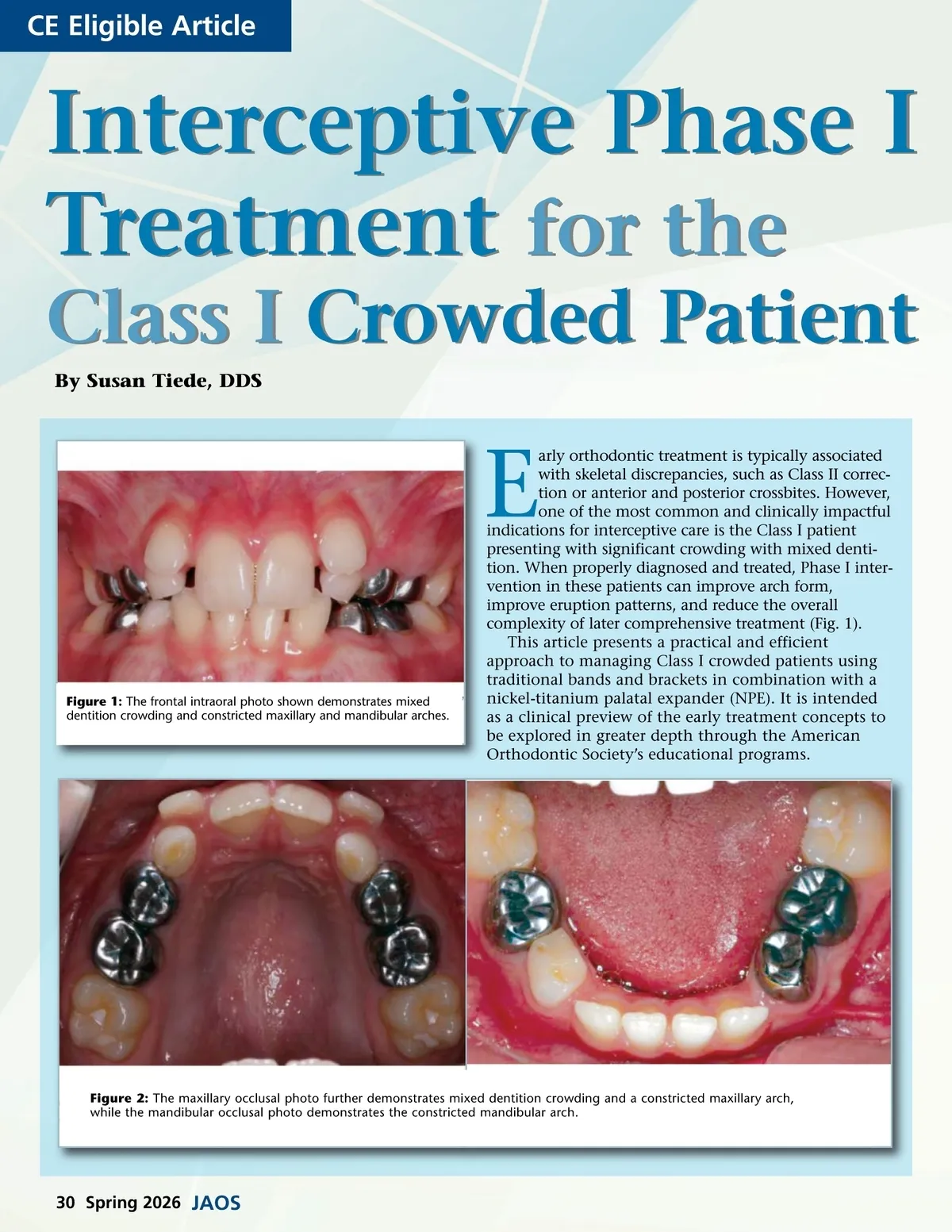
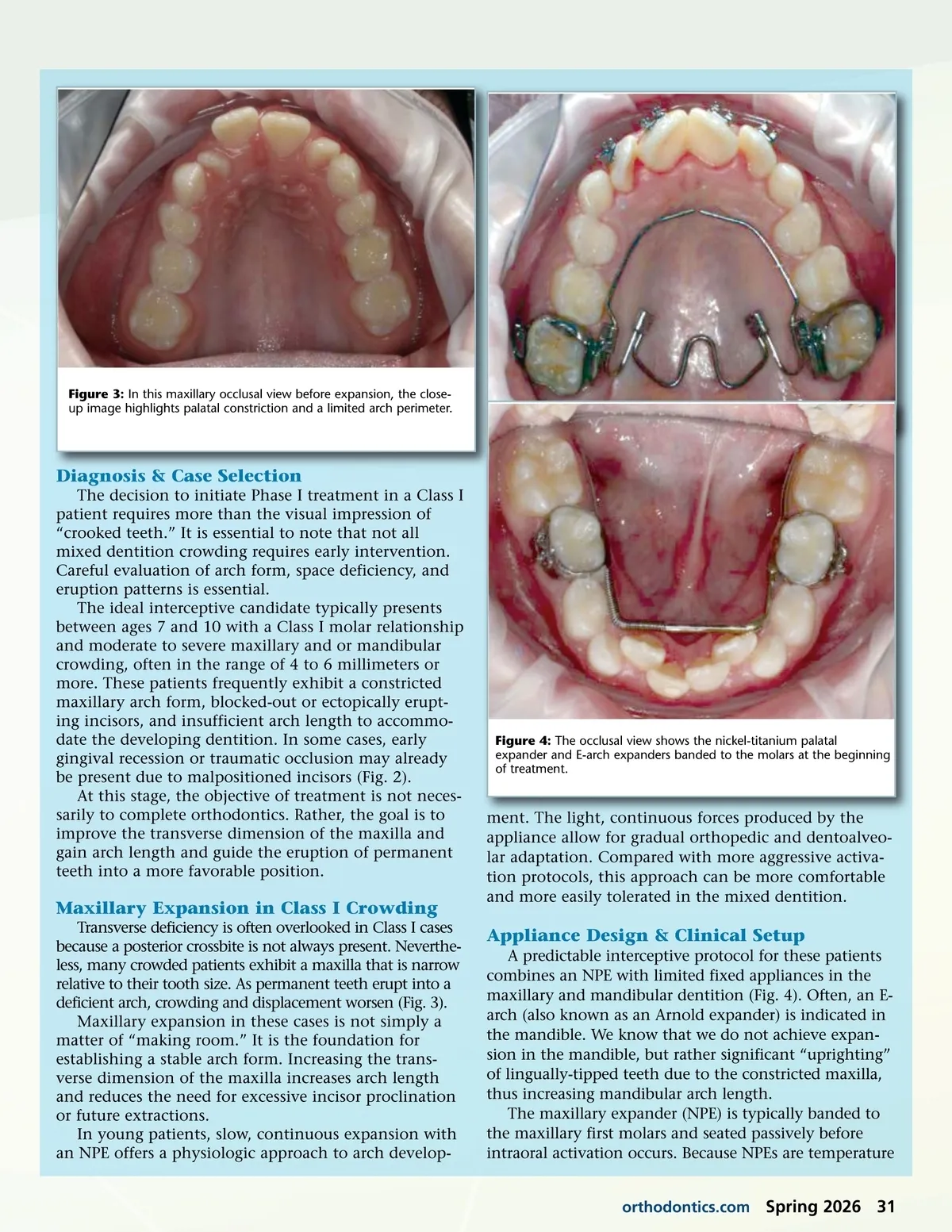
Figure 3: In this maxillary occlusal view before expansion, the close-up image highlights palatal constriction and a limited arch perimeter. Diagnosis & Case Selection The decision to initiate Phase I treatment in a Class I patient requires more than the visual impression of “crooked teeth.” It is essential to note that not all mixed dentition crowding requires early intervention. Careful evaluation of arch form, space deficiency, and eruption patterns is essential. The ideal interceptive candidate typically presents between ages 7 and 10 with a Class I molar relationship and moderate to severe maxillary and or mandibular crowding, often in the range of 4 to 6 millimeters or more. These patients frequently exhibit a constricted maxillary arch form, blocked-out or ectopically erupt-ing incisors, and insufficient arch length to accommo-date the developing dentition. In some cases, early gingival recession or traumatic occlusion may already be present due to malpositioned incisors (Fig. 2). At this stage, the objective of treatment is not neces-sarily to complete orthodontics. Rather, the goal is to improve the transverse dimension of the maxilla and gain arch length and guide the eruption of permanent teeth into a more favorable position. Figure 4: The occlusal view shows the nickel-titanium palatal expander and E-arch expanders banded to the molars at the beginning of treatment. Maxillary Expansion in Class I Crowding Transverse deficiency is often overlooked in Class I cases because a posterior crossbite is not always present. Neverthe-less, many crowded patients exhibit a maxilla that is narrow relative to their tooth size. As permanent teeth erupt into a deficient arch, crowding and displacement worsen (Fig. 3). Maxillary expansion in these cases is not simply a matter of “making room.” It is the foundation for establishing a stable arch form. Increasing the trans-verse dimension of the maxilla increases arch length and reduces the need for excessive incisor proclination or future extractions. In young patients, slow, continuous expansion with an NPE offers a physiologic approach to arch develop-ment. The light, continuous forces produced by the appliance allow for gradual orthopedic and dentoalveo-lar adaptation. Compared with more aggressive activa-tion protocols, this approach can be more comfortable and more easily tolerated in the mixed dentition. Appliance Design & Clinical Setup A predictable interceptive protocol for these patients combines an NPE with limited fixed appliances in the maxillary and mandibular dentition (Fig. 4). Often, an E-arch (also known as an Arnold expander) is indicated in the mandible. We know that we do not achieve expan-sion in the mandible, but rather significant “uprighting” of lingually-tipped teeth due to the constricted maxilla, thus increasing mandibular arch length. The maxillary expander (NPE) is typically banded to the maxillary first molars and seated passively before intraoral activation occurs. Because NPEs are temperature orthodontics.com Spring 2026 31
Journal of the American Orthodontic Society Spring 2026: Page 31