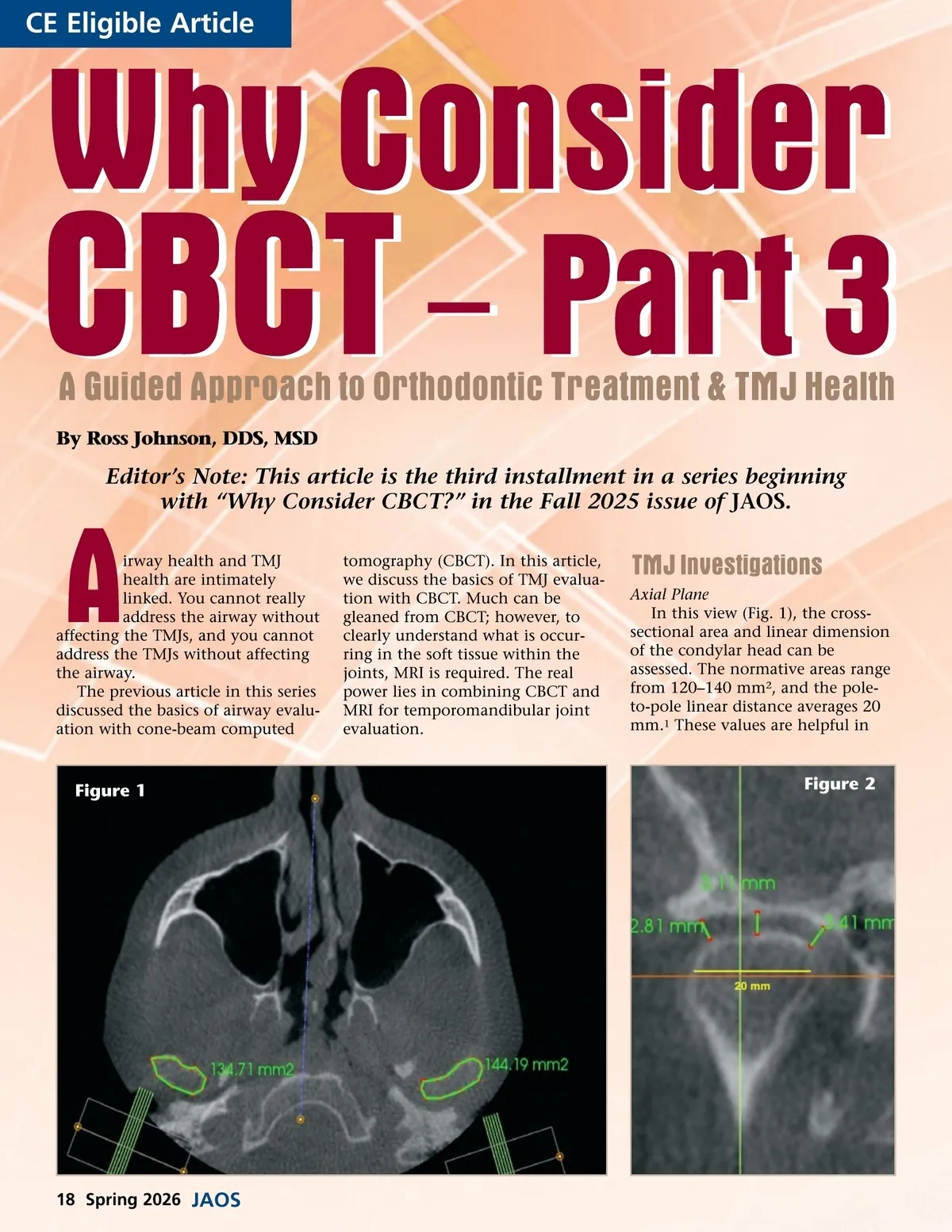
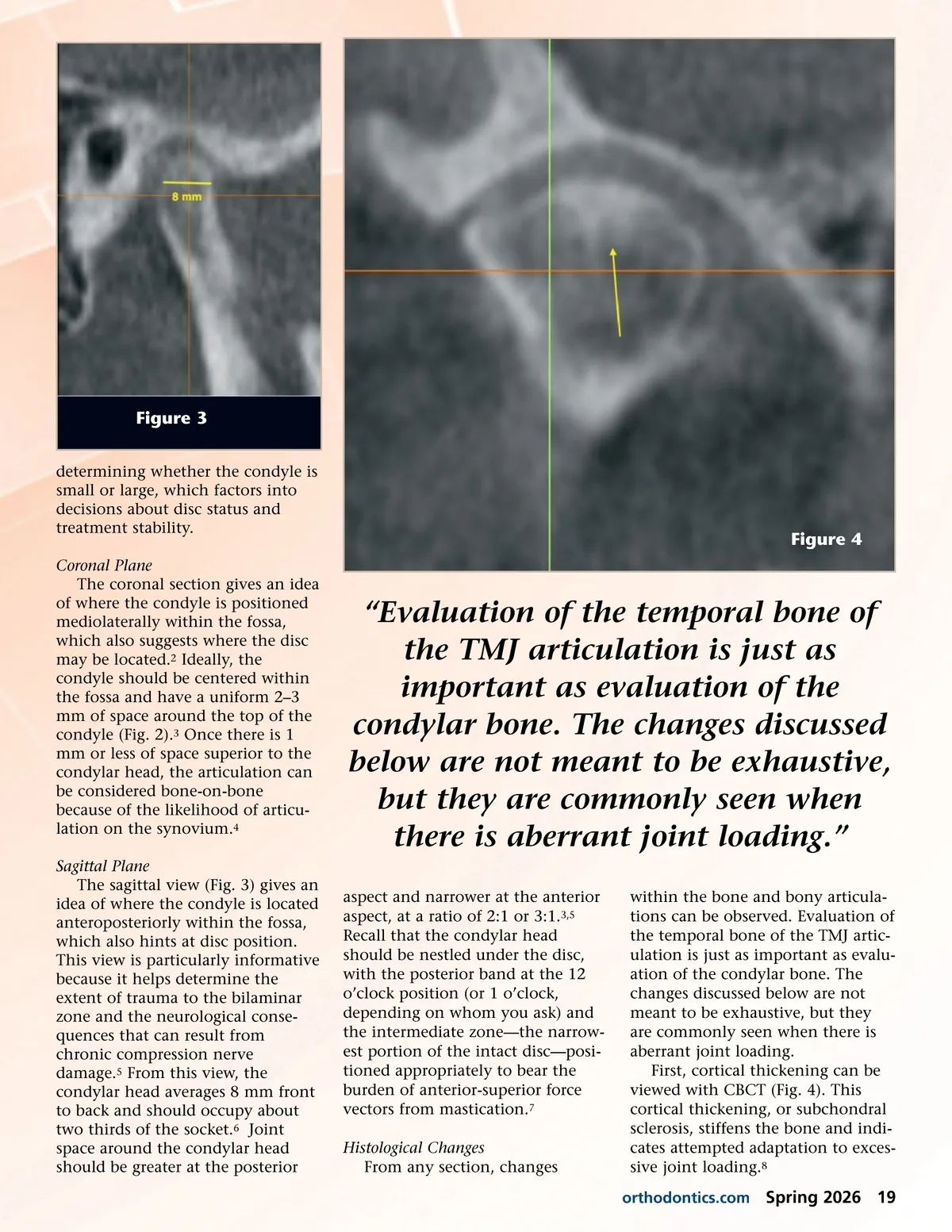
Figure 3 determining whether the condyle is small or large, which factors into decisions about disc status and treatment stability. Coronal Plane The coronal section gives an idea of where the condyle is positioned mediolaterally within the fossa, which also suggests where the disc may be located. 2 Ideally, the condyle should be centered within the fossa and have a uniform 2–3 mm of space around the top of the condyle (Fig. 2). 3 Once there is 1 mm or less of space superior to the condylar head, the articulation can be considered bone-on-bone because of the likelihood of articu-lation on the synovium. 4 Sagittal Plane The sagittal view (Fig. 3) gives an idea of where the condyle is located anteroposteriorly within the fossa, which also hints at disc position. This view is particularly informative because it helps determine the extent of trauma to the bilaminar zone and the neurological conse-quences that can result from chronic compression nerve damage. 5 From this view, the condylar head averages 8 mm front to back and should occupy about two thirds of the socket. 6 Joint space around the condylar head should be greater at the posterior Figure 4 “Evaluation of the temporal bone of the TMJ articulation is just as important as evaluation of the condylar bone. The changes discussed below are not meant to be exhaustive, but they are commonly seen when there is aberrant joint loading.” aspect and narrower at the anterior aspect, at a ratio of 2:1 or 3:1. 3,5 Recall that the condylar head should be nestled under the disc, with the posterior band at the 12 o’clock position (or 1 o’clock, depending on whom you ask) and the intermediate zone—the narrow-est portion of the intact disc—posi-tioned appropriately to bear the burden of anterior-superior force vectors from mastication. 7 Histological Changes From any section, changes within the bone and bony articula-tions can be observed. Evaluation of the temporal bone of the TMJ artic-ulation is just as important as evalu-ation of the condylar bone. The changes discussed below are not meant to be exhaustive, but they are commonly seen when there is aberrant joint loading. First, cortical thickening can be viewed with CBCT (Fig. 4). This cortical thickening, or subchondral sclerosis, stiffens the bone and indi-cates attempted adaptation to exces-sive joint loading. 8 orthodontics.com Spring 2026 19
Journal of the American Orthodontic Society Spring 2026: Page 19