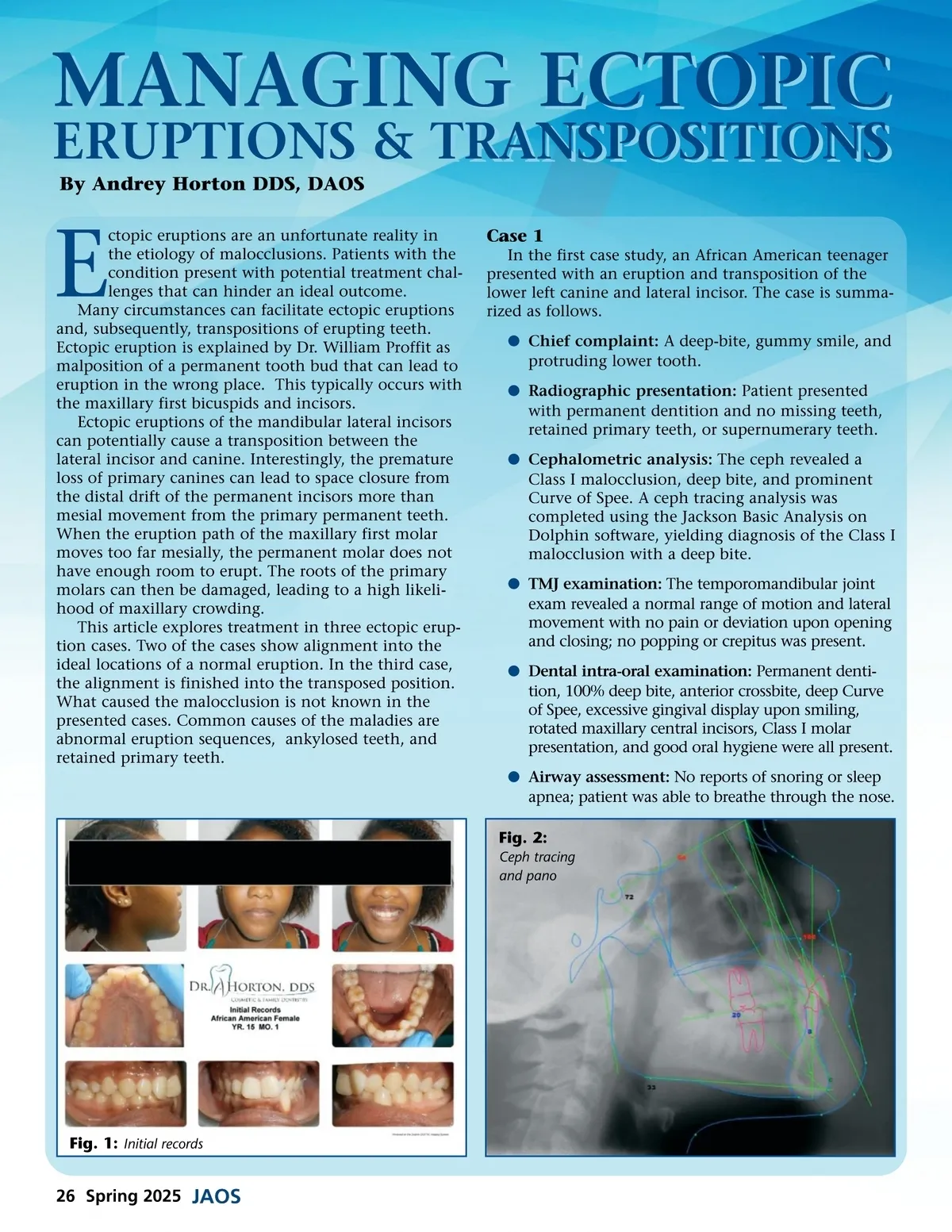
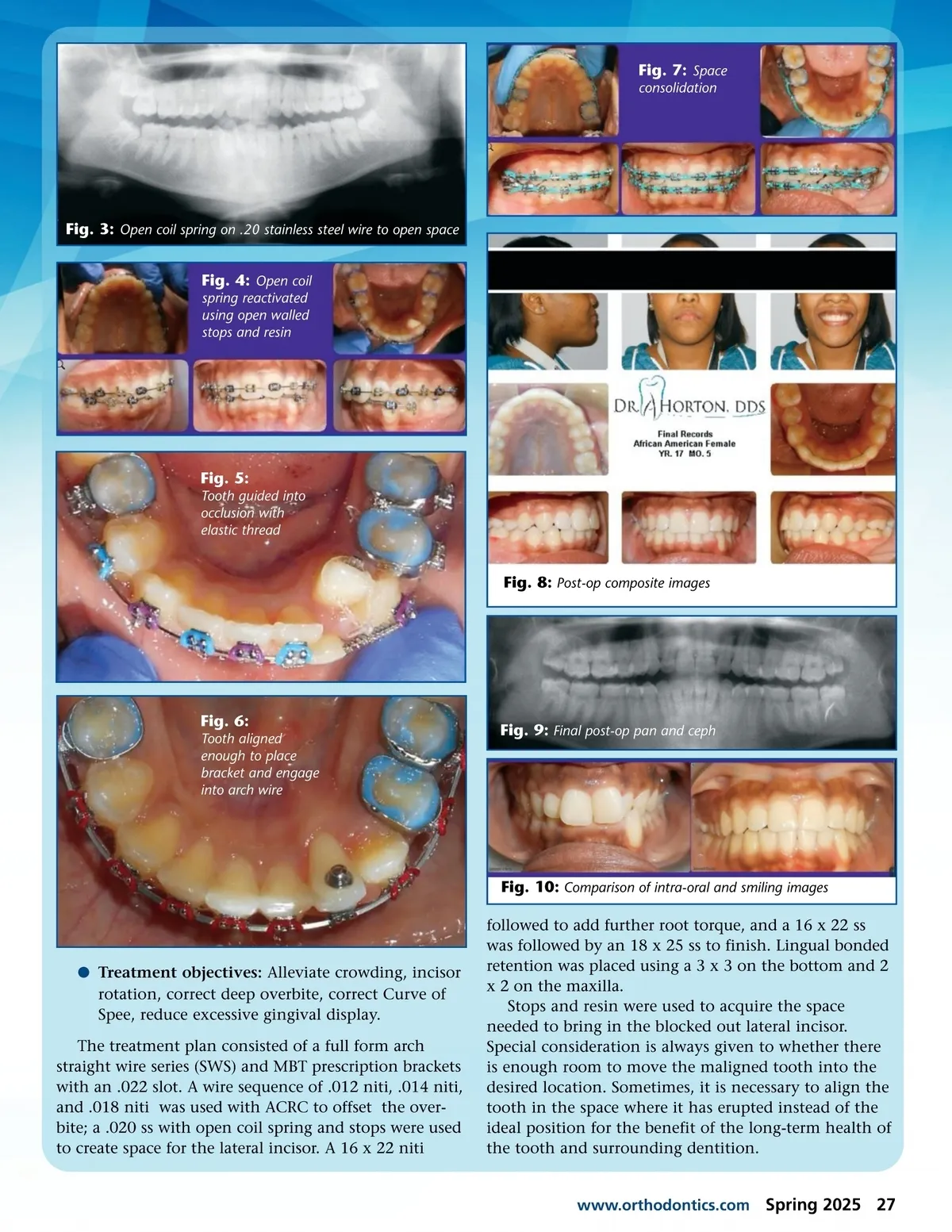
MANAGING ECTOPIC ERUPTIONS & TRANSPOSITIONS By Andrey Horton DDS, DAOS E ctopic eruptions are an unfortunate reality in the etiology of malocclusions. Patients with the condition present with potential treatment chal-lenges that can hinder an ideal outcome. Many circumstances can facilitate ectopic eruptions and, subsequently, transpositions of erupting teeth. Ectopic eruption is explained by Dr. William Proffit as malposition of a permanent tooth bud that can lead to eruption in the wrong place. This typically occurs with the maxillary first bicuspids and incisors. Ectopic eruptions of the mandibular lateral incisors can potentially cause a transposition between the lateral incisor and canine. Interestingly, the premature loss of primary canines can lead to space closure from the distal drift of the permanent incisors more than mesial movement from the primary permanent teeth. When the eruption path of the maxillary first molar moves too far mesially, the permanent molar does not have enough room to erupt. The roots of the primary molars can then be damaged, leading to a high likeli-hood of maxillary crowding. This article explores treatment in three ectopic erup-tion cases. Two of the cases show alignment into the ideal locations of a normal eruption. In the third case, the alignment is finished into the transposed position. What caused the malocclusion is not known in the presented cases. Common causes of the maladies are abnormal eruption sequences, ankylosed teeth, and retained primary teeth. Case 1 In the first case study, an African American teenager presented with an eruption and transposition of the lower left canine and lateral incisor. The case is summa-rized as follows. b Chief complaint: A deep-bite, gummy smile, and protruding lower tooth. b Radiographic presentation: Patient presented with permanent dentition and no missing teeth, retained primary teeth, or supernumerary teeth. b Cephalometric analysis: The ceph revealed a Class I malocclusion, deep bite, and prominent Curve of Spee. A ceph tracing analysis was completed using the Jackson Basic Analysis on Dolphin software, yielding diagnosis of the Class I malocclusion with a deep bite. b TMJ examination: The temporomandibular joint exam revealed a normal range of motion and lateral movement with no pain or deviation upon opening and closing; no popping or crepitus was present. b Dental intra-oral examination: Permanent denti-tion, 100% deep bite, anterior crossbite, deep Curve of Spee, excessive gingival display upon smiling, rotated maxillary central incisors, Class I molar presentation, and good oral hygiene were all present. b Airway assessment: No reports of snoring or sleep apnea; patient was able to breathe through the nose. Fig. 2: Ceph tracing and pano Fig. 1: Initial records 26 Spring 2025 JAOS
Journal of the American Orthodontic Society Spring 2025: Page 26