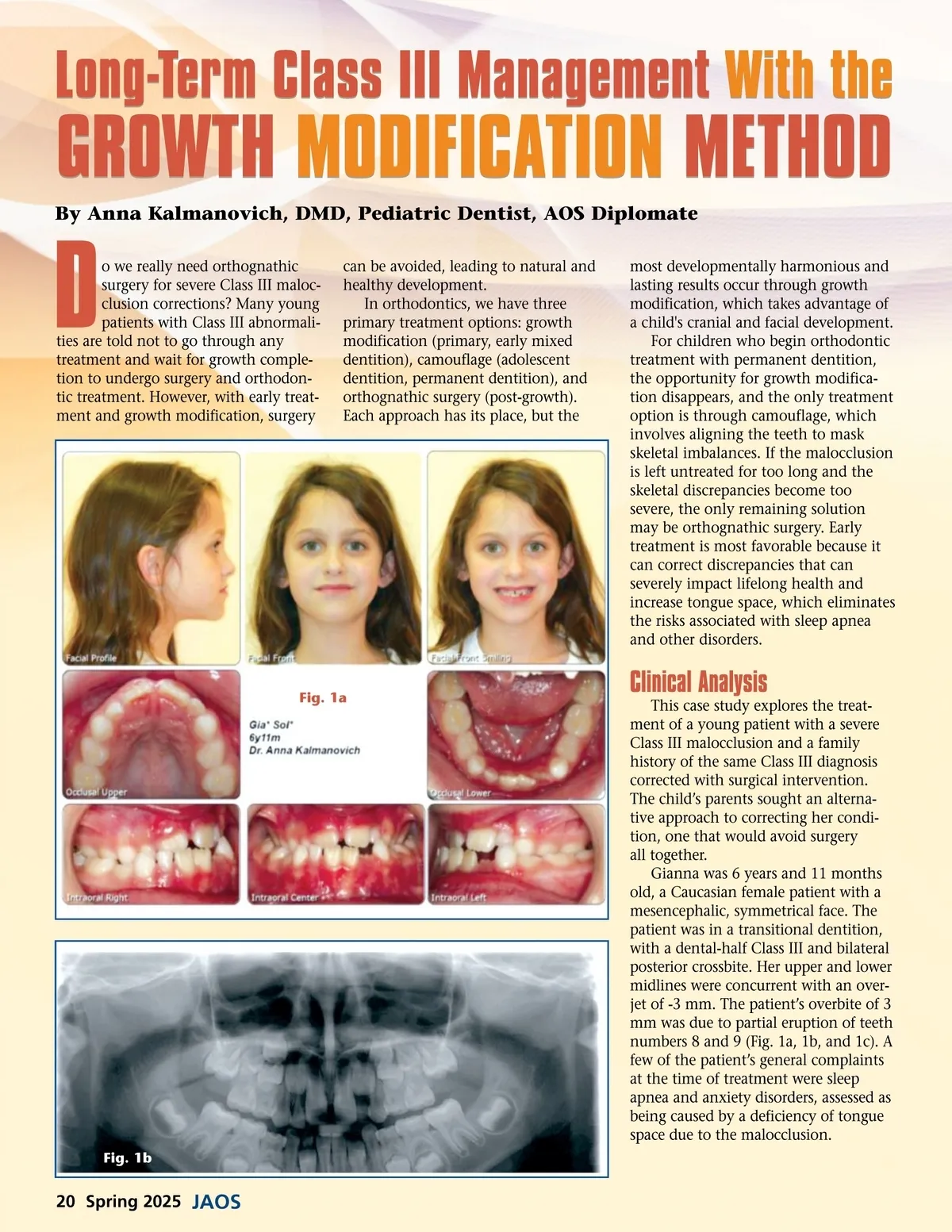
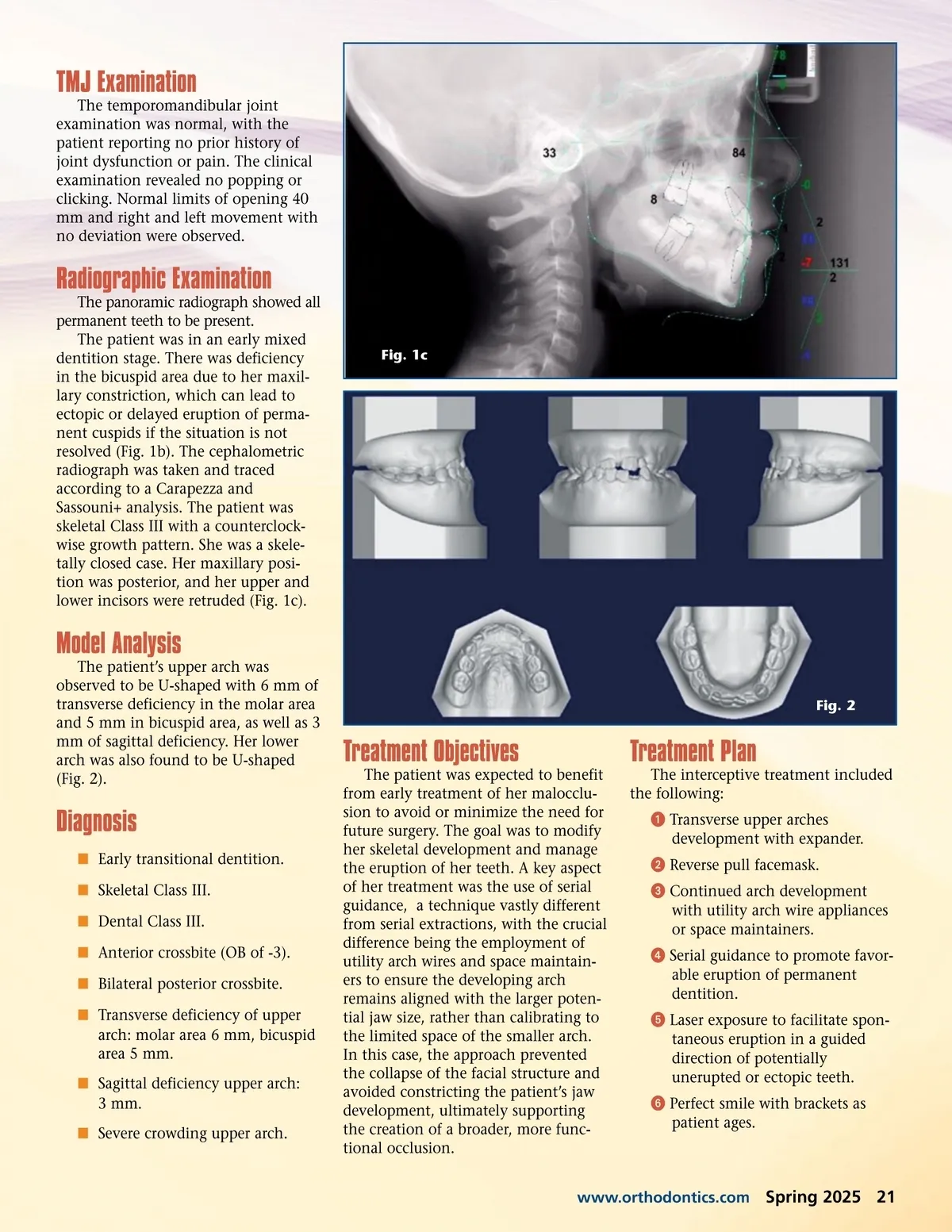
TMJ Examination The temporomandibular joint examination was normal, with the patient reporting no prior history of joint dysfunction or pain. The clinical examination revealed no popping or clicking. Normal limits of opening 40 mm and right and left movement with no deviation were observed. Radiographic Examination The panoramic radiograph showed all permanent teeth to be present. The patient was in an early mixed dentition stage. There was deficiency in the bicuspid area due to her maxil-lary constriction, which can lead to ectopic or delayed eruption of perma-nent cuspids if the situation is not resolved (Fig. 1b). The cephalometric radiograph was taken and traced according to a Carapezza and Sassouni+ analysis. The patient was skeletal Class III with a counterclock-wise growth pattern. She was a skele-tally closed case. Her maxillary posi-tion was posterior, and her upper and lower incisors were retruded (Fig. 1c). Fig. 1c Model Analysis The patient’s upper arch was observed to be U-shaped with 6 mm of transverse deficiency in the molar area and 5 mm in bicuspid area, as well as 3 mm of sagittal deficiency. Her lower arch was also found to be U-shaped (Fig. 2). Fig. 2 Treatment Objectives The patient was expected to benefit from early treatment of her malocclu-sion to avoid or minimize the need for future surgery. The goal was to modify her skeletal development and manage the eruption of her teeth. A key aspect of her treatment was the use of serial guidance, a technique vastly different from serial extractions, with the crucial difference being the employment of utility arch wires and space maintain-ers to ensure the developing arch remains aligned with the larger poten-tial jaw size, rather than calibrating to the limited space of the smaller arch. In this case, the approach prevented the collapse of the facial structure and avoided constricting the patient’s jaw development, ultimately supporting the creation of a broader, more func-tional occlusion. Treatment Plan The interceptive treatment included the following: ᕡ Transverse upper arches development with expander. ᕢ Reverse pull facemask. ᕣ Continued arch development with utility arch wire appliances or space maintainers. ᕤ Serial guidance to promote favor-able eruption of permanent dentition. ᕥ Laser exposure to facilitate spon-taneous eruption in a guided direction of potentially unerupted or ectopic teeth. ᕦ Perfect smile with brackets as patient ages. Diagnosis í Early transitional dentition. í Skeletal Class III. í Dental Class III. í Anterior crossbite (OB of -3). í Bilateral posterior crossbite. í Transverse deficiency of upper arch: molar area 6 mm, bicuspid area 5 mm. í Sagittal deficiency upper arch: 3 mm. í Severe crowding upper arch. www.orthodontics.com Spring 2025 21
Journal of the American Orthodontic Society Spring 2025: Page 21