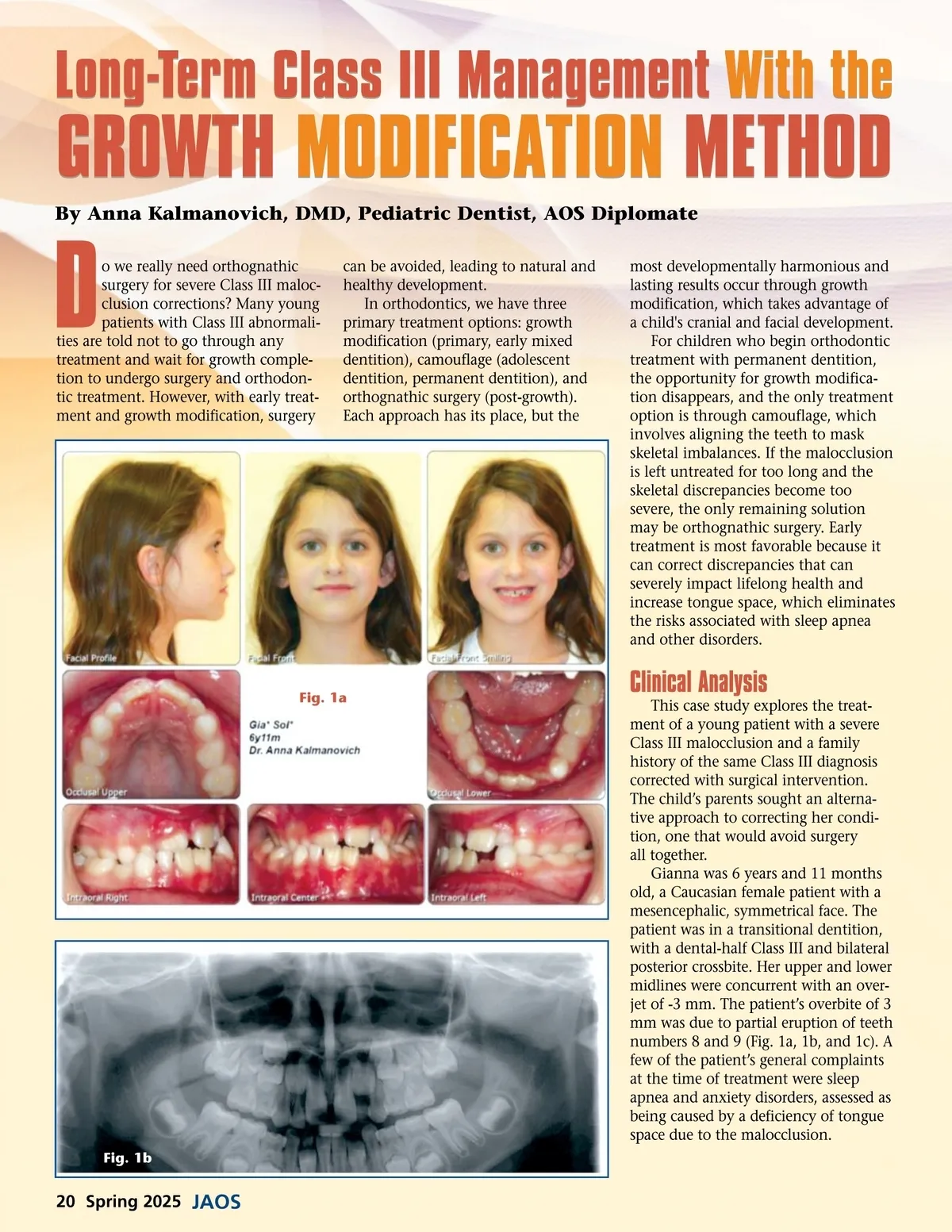
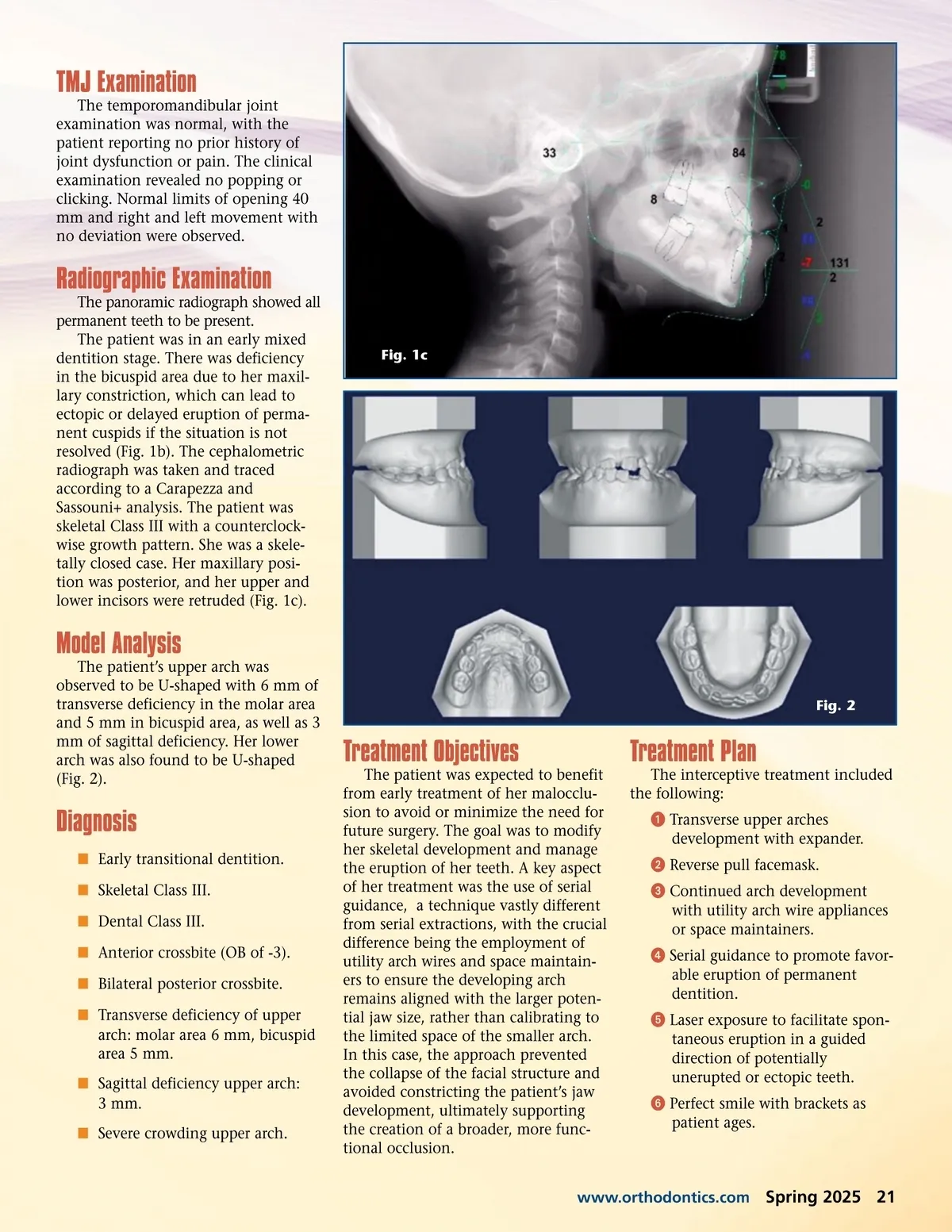
Long-Term Class III Management With the GROWTH MODIFICATION METHOD By Anna Kalmanovich, DMD, Pediatric Dentist, AOS Diplomate D o we really need orthognathic surgery for severe Class III maloc-clusion corrections? Many young patients with Class III abnormali-ties are told not to go through any treatment and wait for growth comple-tion to undergo surgery and orthodon-tic treatment. However, with early treat-ment and growth modification, surgery can be avoided, leading to natural and healthy development. In orthodontics, we have three primary treatment options: growth modification (primary, early mixed dentition), camouflage (adolescent dentition, permanent dentition), and orthognathic surgery (post-growth). Each approach has its place, but the most developmentally harmonious and lasting results occur through growth modification, which takes advantage of a child's cranial and facial development. For children who begin orthodontic treatment with permanent dentition, the opportunity for growth modifica-tion disappears, and the only treatment option is through camouflage, which involves aligning the teeth to mask skeletal imbalances. If the malocclusion is left untreated for too long and the skeletal discrepancies become too severe, the only remaining solution may be orthognathic surgery. Early treatment is most favorable because it can correct discrepancies that can severely impact lifelong health and increase tongue space, which eliminates the risks associated with sleep apnea and other disorders. Fig. 1a Clinical Analysis This case study explores the treat-ment of a young patient with a severe Class III malocclusion and a family history of the same Class III diagnosis corrected with surgical intervention. The child’s parents sought an alterna-tive approach to correcting her condi-tion, one that would avoid surgery all together. Gianna was 6 years and 11 months old, a Caucasian female patient with a mesencephalic, symmetrical face. The patient was in a transitional dentition, with a dental-half Class III and bilateral posterior crossbite. Her upper and lower midlines were concurrent with an over-jet of -3 mm. The patient’s overbite of 3 mm was due to partial eruption of teeth numbers 8 and 9 (Fig. 1a, 1b, and 1c). A few of the patient’s general complaints at the time of treatment were sleep apnea and anxiety disorders, assessed as being caused by a deficiency of tongue space due to the malocclusion. Fig. 1b 20 Spring 2025 JAOS
Journal of the American Orthodontic Society Spring 2025: Page 20