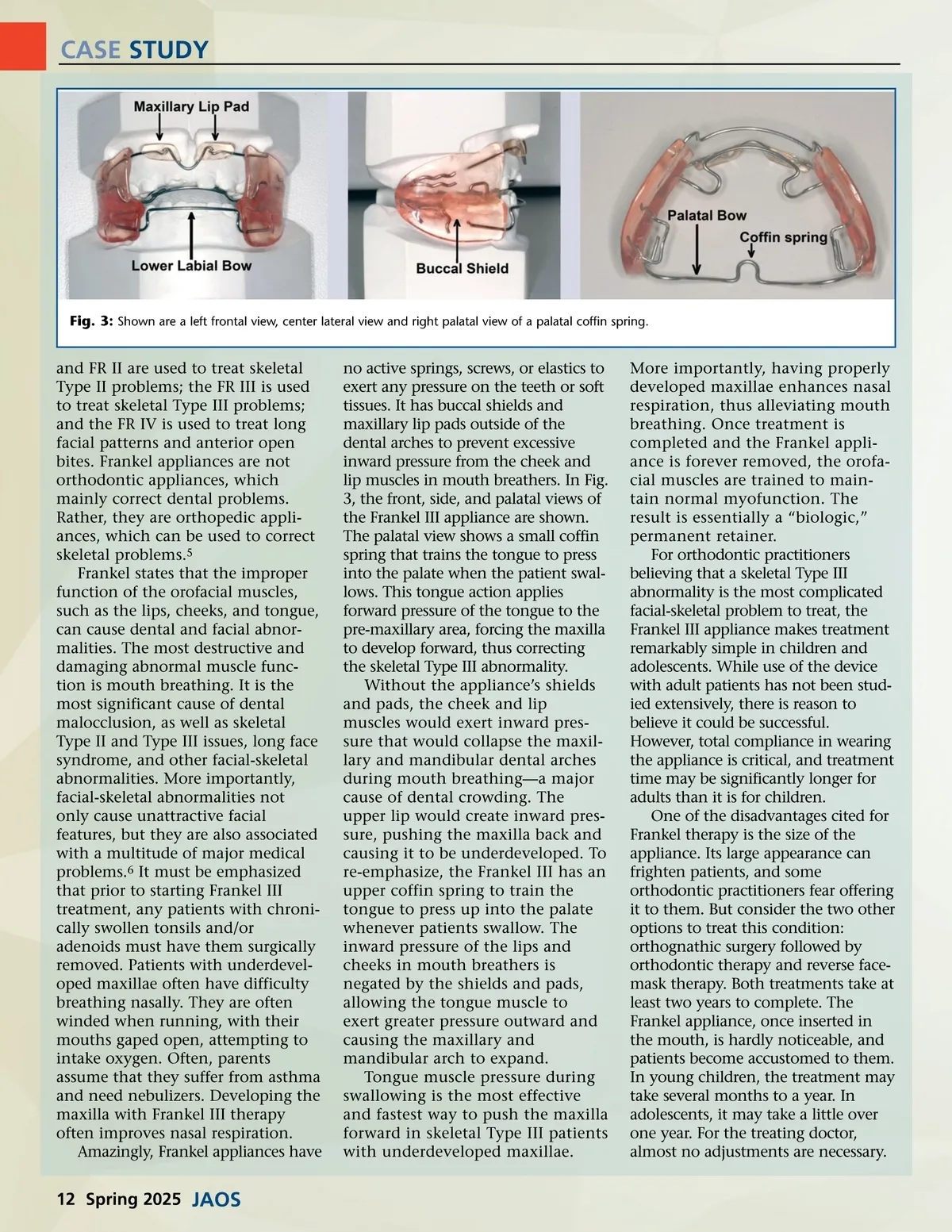
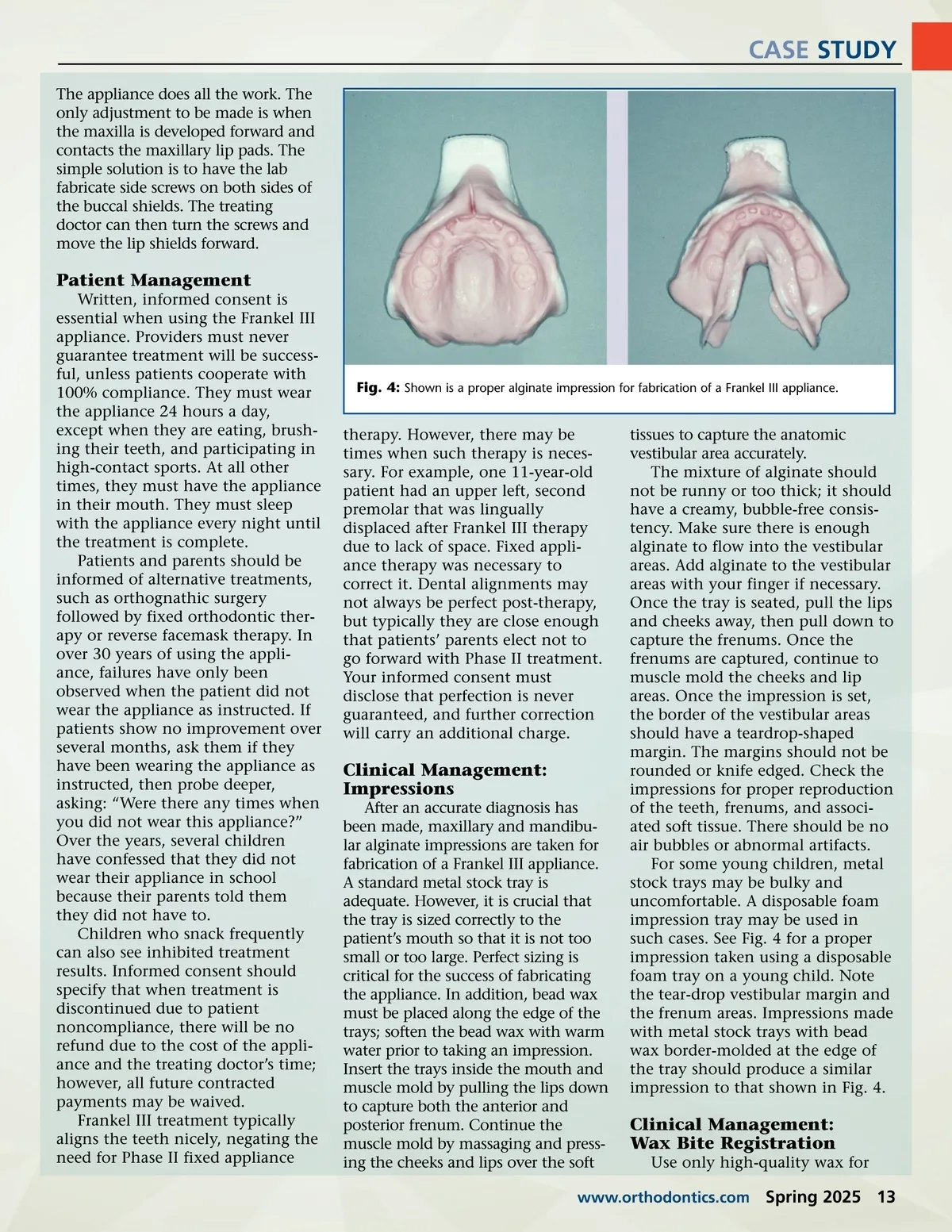
CASE STUDY The appliance does all the work. The only adjustment to be made is when the maxilla is developed forward and contacts the maxillary lip pads. The simple solution is to have the lab fabricate side screws on both sides of the buccal shields. The treating doctor can then turn the screws and move the lip shields forward. Patient Management Written, informed consent is essential when using the Frankel III appliance. Providers must never guarantee treatment will be success-ful, unless patients cooperate with 100% compliance. They must wear the appliance 24 hours a day, except when they are eating, brush-ing their teeth, and participating in high-contact sports. At all other times, they must have the appliance in their mouth. They must sleep with the appliance every night until the treatment is complete. Patients and parents should be informed of alternative treatments, such as orthognathic surgery followed by fixed orthodontic ther-apy or reverse facemask therapy. In over 30 years of using the appli-ance, failures have only been observed when the patient did not wear the appliance as instructed. If patients show no improvement over several months, ask them if they have been wearing the appliance as instructed, then probe deeper, asking: “Were there any times when you did not wear this appliance?” Over the years, several children have confessed that they did not wear their appliance in school because their parents told them they did not have to. Children who snack frequently can also see inhibited treatment results. Informed consent should specify that when treatment is discontinued due to patient noncompliance, there will be no refund due to the cost of the appli-ance and the treating doctor’s time; however, all future contracted payments may be waived. Frankel III treatment typically aligns the teeth nicely, negating the need for Phase II fixed appliance Fig. 4: Shown is a proper alginate impression for fabrication of a Frankel III appliance. therapy. However, there may be times when such therapy is neces-sary. For example, one 11-year-old patient had an upper left, second premolar that was lingually displaced after Frankel III therapy due to lack of space. Fixed appli-ance therapy was necessary to correct it. Dental alignments may not always be perfect post-therapy, but typically they are close enough that patients’ parents elect not to go forward with Phase II treatment. Your informed consent must disclose that perfection is never guaranteed, and further correction will carry an additional charge. Clinical Management: Impressions After an accurate diagnosis has been made, maxillary and mandibu-lar alginate impressions are taken for fabrication of a Frankel III appliance. A standard metal stock tray is adequate. However, it is crucial that the tray is sized correctly to the patient’s mouth so that it is not too small or too large. Perfect sizing is critical for the success of fabricating the appliance. In addition, bead wax must be placed along the edge of the trays; soften the bead wax with warm water prior to taking an impression. Insert the trays inside the mouth and muscle mold by pulling the lips down to capture both the anterior and posterior frenum. Continue the muscle mold by massaging and press-ing the cheeks and lips over the soft tissues to capture the anatomic vestibular area accurately. The mixture of alginate should not be runny or too thick; it should have a creamy, bubble-free consis-tency. Make sure there is enough alginate to flow into the vestibular areas. Add alginate to the vestibular areas with your finger if necessary. Once the tray is seated, pull the lips and cheeks away, then pull down to capture the frenums. Once the frenums are captured, continue to muscle mold the cheeks and lip areas. Once the impression is set, the border of the vestibular areas should have a teardrop-shaped margin. The margins should not be rounded or knife edged. Check the impressions for proper reproduction of the teeth, frenums, and associ-ated soft tissue. There should be no air bubbles or abnormal artifacts. For some young children, metal stock trays may be bulky and uncomfortable. A disposable foam impression tray may be used in such cases. See Fig. 4 for a proper impression taken using a disposable foam tray on a young child. Note the tear-drop vestibular margin and the frenum areas. Impressions made with metal stock trays with bead wax border-molded at the edge of the tray should produce a similar impression to that shown in Fig. 4. Clinical Management: Wax Bite Registration Use only high-quality wax for www.orthodontics.com Spring 2025 13
Journal of the American Orthodontic Society Spring 2025: Page 13