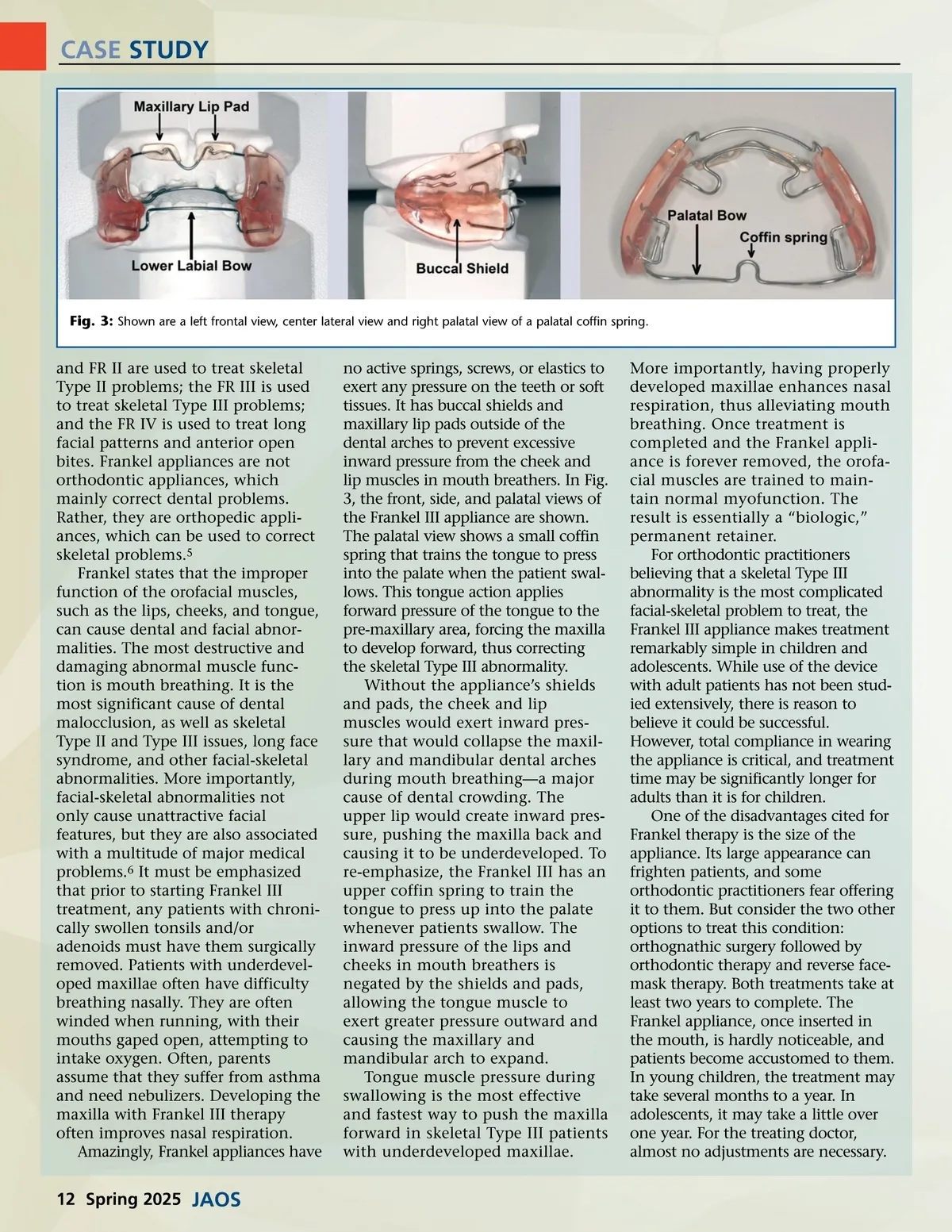
CASE STUDY Fig. 3: Shown are a left frontal view, center lateral view and right palatal view of a palatal coffin spring. and FR II are used to treat skeletal Type II problems; the FR III is used to treat skeletal Type III problems; and the FR IV is used to treat long facial patterns and anterior open bites. Frankel appliances are not orthodontic appliances, which mainly correct dental problems. Rather, they are orthopedic appli-ances, which can be used to correct skeletal problems. 5 Frankel states that the improper function of the orofacial muscles, such as the lips, cheeks, and tongue, can cause dental and facial abnor-malities. The most destructive and damaging abnormal muscle func-tion is mouth breathing. It is the most significant cause of dental malocclusion, as well as skeletal Type II and Type III issues, long face syndrome, and other facial-skeletal abnormalities. More importantly, facial-skeletal abnormalities not only cause unattractive facial features, but they are also associated with a multitude of major medical problems. 6 It must be emphasized that prior to starting Frankel III treatment, any patients with chroni-cally swollen tonsils and/or adenoids must have them surgically removed. Patients with underdevel-oped maxillae often have difficulty breathing nasally. They are often winded when running, with their mouths gaped open, attempting to intake oxygen. Often, parents assume that they suffer from asthma and need nebulizers. Developing the maxilla with Frankel III therapy often improves nasal respiration. Amazingly, Frankel appliances have no active springs, screws, or elastics to exert any pressure on the teeth or soft tissues. It has buccal shields and maxillary lip pads outside of the dental arches to prevent excessive inward pressure from the cheek and lip muscles in mouth breathers. In Fig. 3, the front, side, and palatal views of the Frankel III appliance are shown. The palatal view shows a small coffin spring that trains the tongue to press into the palate when the patient swal-lows. This tongue action applies forward pressure of the tongue to the pre-maxillary area, forcing the maxilla to develop forward, thus correcting the skeletal Type III abnormality. Without the appliance’s shields and pads, the cheek and lip muscles would exert inward pres-sure that would collapse the maxil-lary and mandibular dental arches during mouth breathing—a major cause of dental crowding. The upper lip would create inward pres-sure, pushing the maxilla back and causing it to be underdeveloped. To re-emphasize, the Frankel III has an upper coffin spring to train the tongue to press up into the palate whenever patients swallow. The inward pressure of the lips and cheeks in mouth breathers is negated by the shields and pads, allowing the tongue muscle to exert greater pressure outward and causing the maxillary and mandibular arch to expand. Tongue muscle pressure during swallowing is the most effective and fastest way to push the maxilla forward in skeletal Type III patients with underdeveloped maxillae. More importantly, having properly developed maxillae enhances nasal respiration, thus alleviating mouth breathing. Once treatment is completed and the Frankel appli-ance is forever removed, the orofa-cial muscles are trained to main-tain normal myofunction. The result is essentially a “biologic,” permanent retainer. For orthodontic practitioners believing that a skeletal Type III abnormality is the most complicated facial-skeletal problem to treat, the Frankel III appliance makes treatment remarkably simple in children and adolescents. While use of the device with adult patients has not been stud-ied extensively, there is reason to believe it could be successful. However, total compliance in wearing the appliance is critical, and treatment time may be significantly longer for adults than it is for children. One of the disadvantages cited for Frankel therapy is the size of the appliance. Its large appearance can frighten patients, and some orthodontic practitioners fear offering it to them. But consider the two other options to treat this condition: orthognathic surgery followed by orthodontic therapy and reverse face-mask therapy. Both treatments take at least two years to complete. The Frankel appliance, once inserted in the mouth, is hardly noticeable, and patients become accustomed to them. In young children, the treatment may take several months to a year. In adolescents, it may take a little over one year. For the treating doctor, almost no adjustments are necessary. 12 Spring 2025 JAOS
Journal of the American Orthodontic Society Spring 2025: Page 12