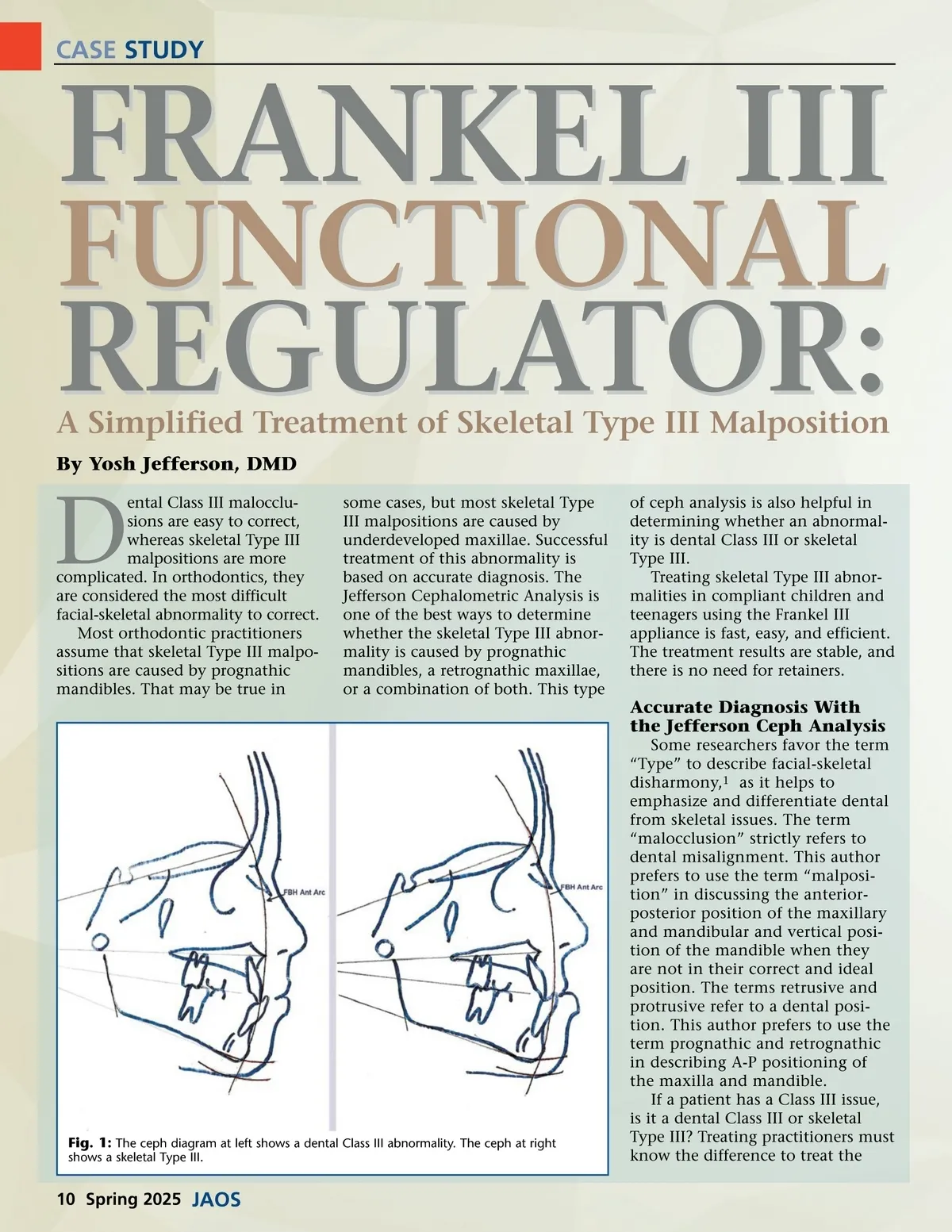
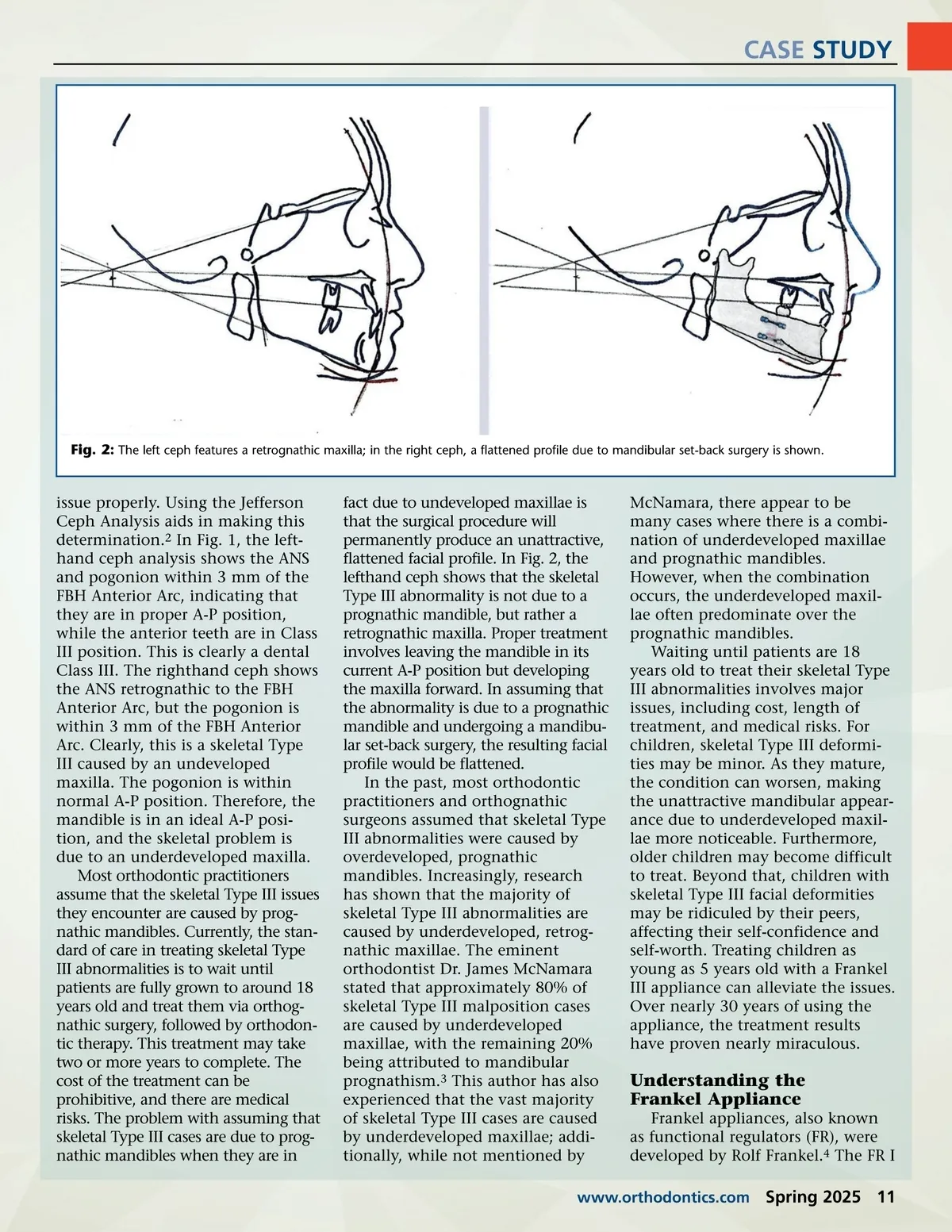
CASE STUDY Fig. 2: The left ceph features a retrognathic maxilla; in the right ceph, a flattened profile due to mandibular set-back surgery is shown. issue properly. Using the Jefferson Ceph Analysis aids in making this determination. 2 In Fig. 1, the left-hand ceph analysis shows the ANS and pogonion within 3 mm of the FBH Anterior Arc, indicating that they are in proper A-P position, while the anterior teeth are in Class III position. This is clearly a dental Class III. The righthand ceph shows the ANS retrognathic to the FBH Anterior Arc, but the pogonion is within 3 mm of the FBH Anterior Arc. Clearly, this is a skeletal Type III caused by an undeveloped maxilla. The pogonion is within normal A-P position. Therefore, the mandible is in an ideal A-P posi-tion, and the skeletal problem is due to an underdeveloped maxilla. Most orthodontic practitioners assume that the skeletal Type III issues they encounter are caused by prog-nathic mandibles. Currently, the stan-dard of care in treating skeletal Type III abnormalities is to wait until patients are fully grown to around 18 years old and treat them via orthog-nathic surgery, followed by orthodon-tic therapy. This treatment may take two or more years to complete. The cost of the treatment can be prohibitive, and there are medical risks. The problem with assuming that skeletal Type III cases are due to prog-nathic mandibles when they are in fact due to undeveloped maxillae is that the surgical procedure will permanently produce an unattractive, flattened facial profile. In Fig. 2, the lefthand ceph shows that the skeletal Type III abnormality is not due to a prognathic mandible, but rather a retrognathic maxilla. Proper treatment involves leaving the mandible in its current A-P position but developing the maxilla forward. In assuming that the abnormality is due to a prognathic mandible and undergoing a mandibu-lar set-back surgery, the resulting facial profile would be flattened. In the past, most orthodontic practitioners and orthognathic surgeons assumed that skeletal Type III abnormalities were caused by overdeveloped, prognathic mandibles. Increasingly, research has shown that the majority of skeletal Type III abnormalities are caused by underdeveloped, retrog-nathic maxillae. The eminent orthodontist Dr. James McNamara stated that approximately 80% of skeletal Type III malposition cases are caused by underdeveloped maxillae, with the remaining 20% being attributed to mandibular prognathism. 3 This author has also experienced that the vast majority of skeletal Type III cases are caused by underdeveloped maxillae; addi-tionally, while not mentioned by McNamara, there appear to be many cases where there is a combi-nation of underdeveloped maxillae and prognathic mandibles. However, when the combination occurs, the underdeveloped maxil-lae often predominate over the prognathic mandibles. Waiting until patients are 18 years old to treat their skeletal Type III abnormalities involves major issues, including cost, length of treatment, and medical risks. For children, skeletal Type III deformi-ties may be minor. As they mature, the condition can worsen, making the unattractive mandibular appear-ance due to underdeveloped maxil-lae more noticeable. Furthermore, older children may become difficult to treat. Beyond that, children with skeletal Type III facial deformities may be ridiculed by their peers, affecting their self-confidence and self-worth. Treating children as young as 5 years old with a Frankel III appliance can alleviate the issues. Over nearly 30 years of using the appliance, the treatment results have proven nearly miraculous. Understanding the Frankel Appliance Frankel appliances, also known as functional regulators (FR), were developed by Rolf Frankel. 4 The FR I www.orthodontics.com Spring 2025 11
Journal of the American Orthodontic Society Spring 2025: Page 11