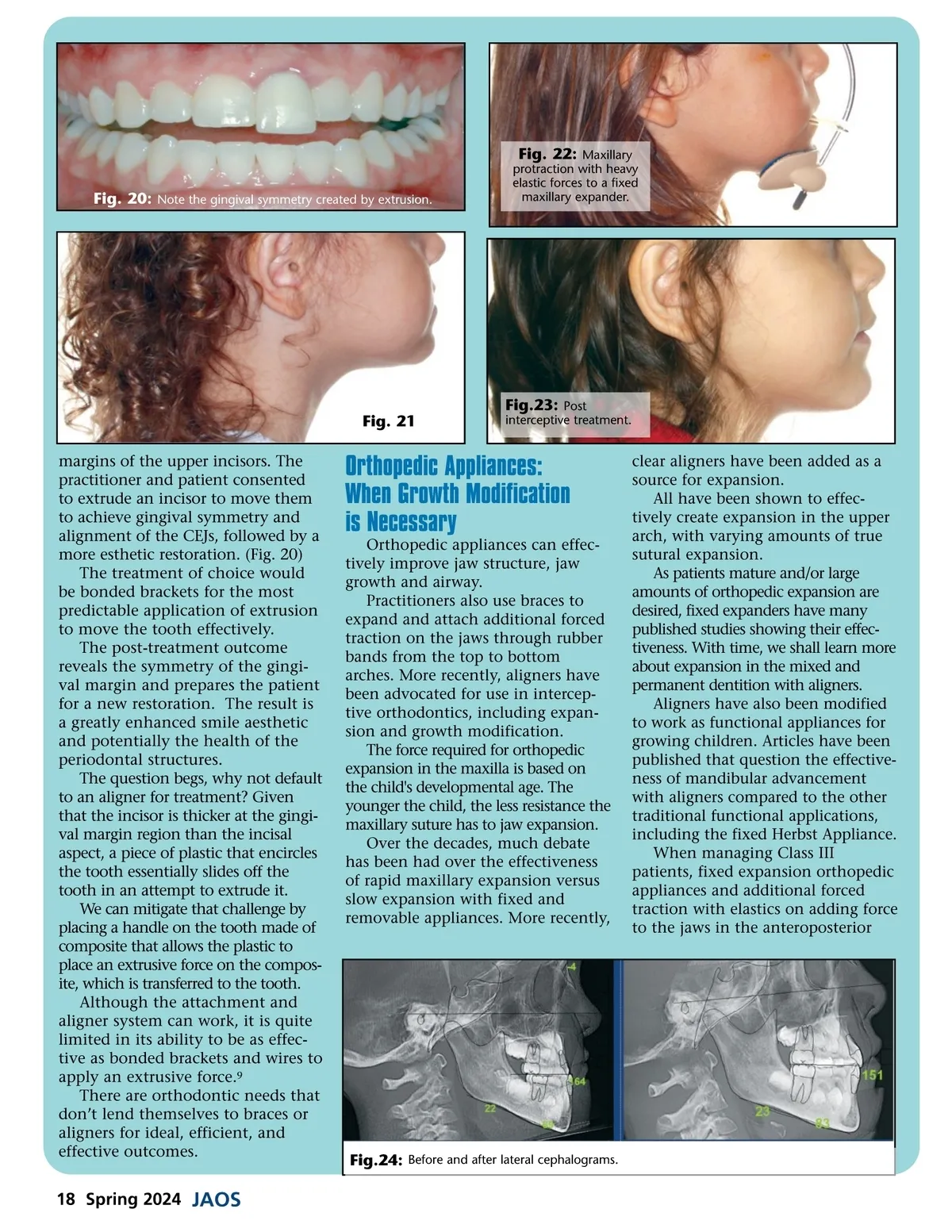
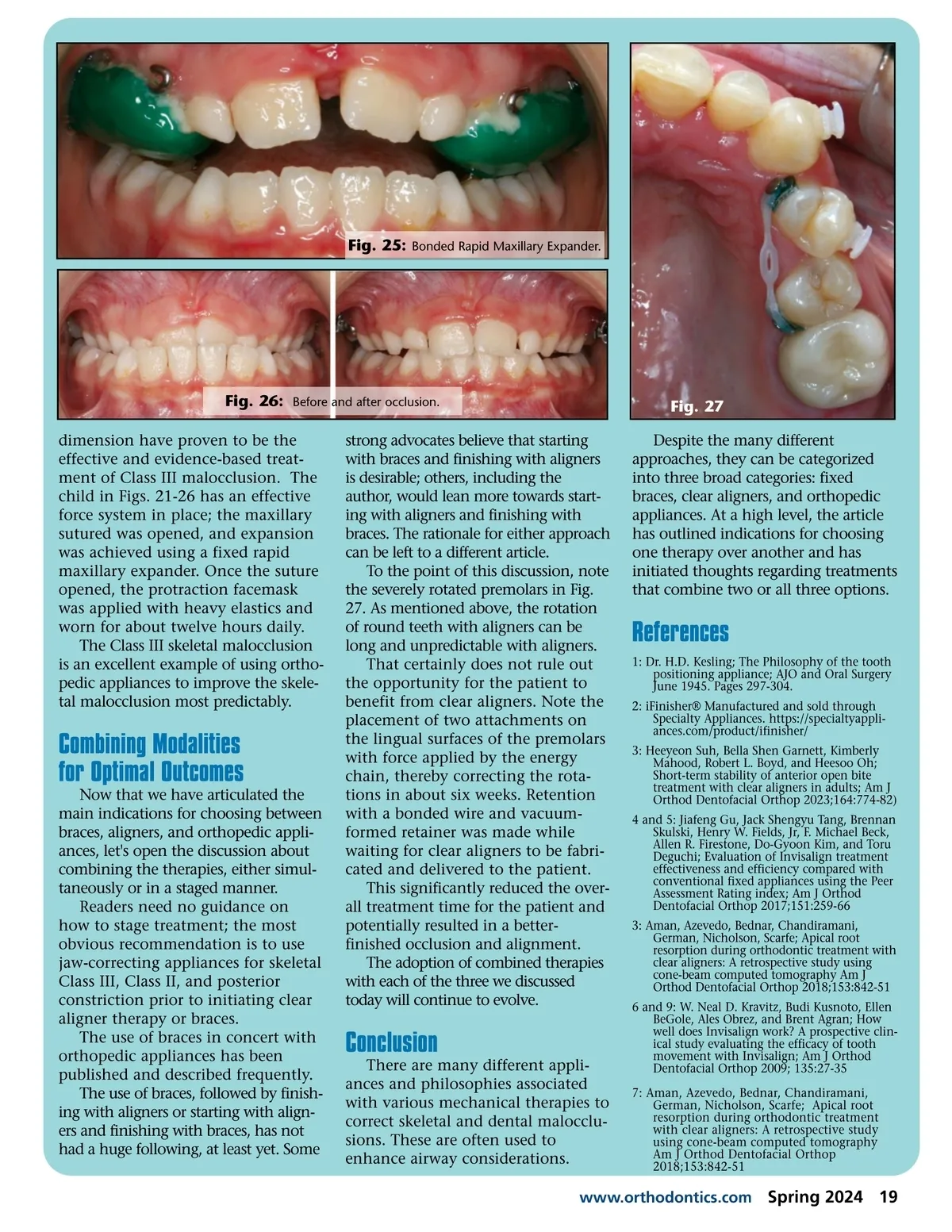
Fig. 20: Note the gingival symmetry created by extrusion. Fig. 22: Maxillary protraction with heavy elastic forces to a fixed maxillary expander. Fig.23: Post Fig. 21 margins of the upper incisors. The practitioner and patient consented to extrude an incisor to move them to achieve gingival symmetry and alignment of the CEJs, followed by a more esthetic restoration. (Fig. 20) The treatment of choice would be bonded brackets for the most predictable application of extrusion to move the tooth effectively. The post-treatment outcome reveals the symmetry of the gingi-val margin and prepares the patient for a new restoration. The result is a greatly enhanced smile aesthetic and potentially the health of the periodontal structures. The question begs, why not default to an aligner for treatment? Given that the incisor is thicker at the gingi-val margin region than the incisal aspect, a piece of plastic that encircles the tooth essentially slides off the tooth in an attempt to extrude it. We can mitigate that challenge by placing a handle on the tooth made of composite that allows the plastic to place an extrusive force on the compos-ite, which is transferred to the tooth. Although the attachment and aligner system can work, it is quite limited in its ability to be as effec-tive as bonded brackets and wires to apply an extrusive force. 9 There are orthodontic needs that don’t lend themselves to braces or aligners for ideal, efficient, and effective outcomes. interceptive treatment. Orthopedic Appliances: When Growth Modification is Necessary Orthopedic appliances can effec-tively improve jaw structure, jaw growth and airway. Practitioners also use braces to expand and attach additional forced traction on the jaws through rubber bands from the top to bottom arches. More recently, aligners have been advocated for use in intercep-tive orthodontics, including expan-sion and growth modification. The force required for orthopedic expansion in the maxilla is based on the child's developmental age. The younger the child, the less resistance the maxillary suture has to jaw expansion. Over the decades, much debate has been had over the effectiveness of rapid maxillary expansion versus slow expansion with fixed and removable appliances. More recently, clear aligners have been added as a source for expansion. All have been shown to effec-tively create expansion in the upper arch, with varying amounts of true sutural expansion. As patients mature and/or large amounts of orthopedic expansion are desired, fixed expanders have many published studies showing their effec-tiveness. With time, we shall learn more about expansion in the mixed and permanent dentition with aligners. Aligners have also been modified to work as functional appliances for growing children. Articles have been published that question the effective-ness of mandibular advancement with aligners compared to the other traditional functional applications, including the fixed Herbst Appliance. When managing Class III patients, fixed expansion orthopedic appliances and additional forced traction with elastics on adding force to the jaws in the anteroposterior Fig.24: Before and after lateral cephalograms. 18 Spring 2024 JAOS
Journal of the American Orthodontic Society Spring 2024: Page 18