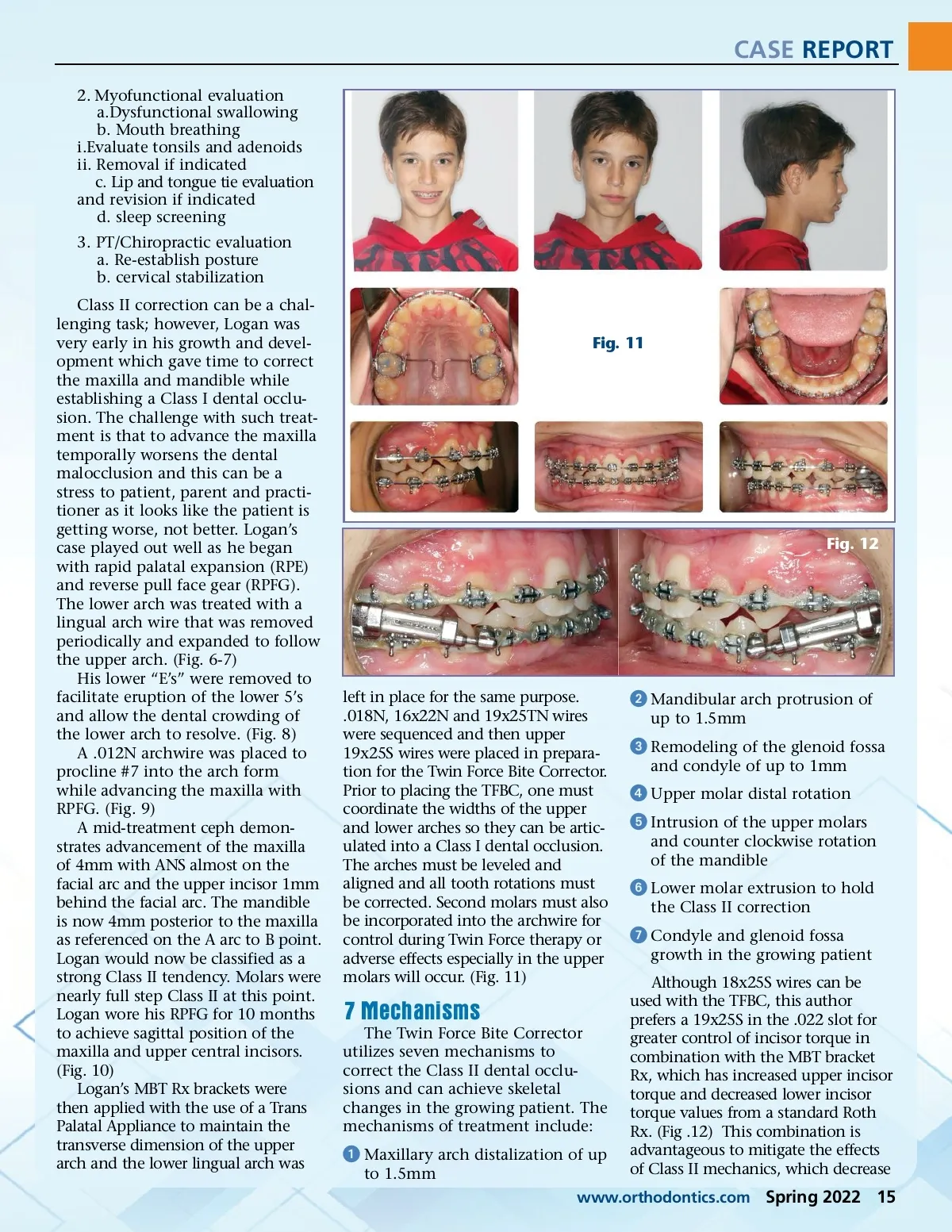
CASE REPORT 2. Myofunctional evaluation a.Dysfunctional swallowing b. Mouth breathing i.Evaluate tonsils and adenoids ii. Removal if indicated c. Lip and tongue tie evaluation and revision if indicated d. sleep screening 3. PT/Chiropractic evaluation a. Re-establish posture b. cervical stabilization Class II correction can be a chal-lenging task; however, Logan was very early in his growth and devel-opment which gave time to correct the maxilla and mandible while establishing a Class I dental occlu-sion. The challenge with such treat-ment is that to advance the maxilla temporally worsens the dental malocclusion and this can be a stress to patient, parent and practi-tioner as it looks like the patient is getting worse, not better. Logan’s case played out well as he began with rapid palatal expansion (RPE) and reverse pull face gear (RPFG). The lower arch was treated with a lingual arch wire that was removed periodically and expanded to follow the upper arch. (Fig. 6-7) His lower “E’s” were removed to facilitate eruption of the lower 5’s and allow the dental crowding of the lower arch to resolve. (Fig. 8) A .012N archwire was placed to procline #7 into the arch form while advancing the maxilla with RPFG. (Fig. 9) A mid-treatment ceph demon-strates advancement of the maxilla of 4mm with ANS almost on the facial arc and the upper incisor 1mm behind the facial arc. The mandible is now 4mm posterior to the maxilla as referenced on the A arc to B point. Logan would now be classified as a strong Class II tendency. Molars were nearly full step Class II at this point. Logan wore his RPFG for 10 months to achieve sagittal position of the maxilla and upper central incisors. (Fig. 10) Logan’s MBT Rx brackets were then applied with the use of a Trans Palatal Appliance to maintain the transverse dimension of the upper arch and the lower lingual arch was Fig. 11 Fig. 12 left in place for the same purpose. .018N, 16x22N and 19x25TN wires were sequenced and then upper 19x25S wires were placed in prepara-tion for the Twin Force Bite Corrector. Prior to placing the TFBC, one must coordinate the widths of the upper and lower arches so they can be artic-ulated into a Class I dental occlusion. The arches must be leveled and aligned and all tooth rotations must be corrected. Second molars must also be incorporated into the archwire for control during Twin Force therapy or adverse effects especially in the upper molars will occur. (Fig. 11) ᕢ Mandibular arch protrusion of up to 1.5mm ᕣ Remodeling of the glenoid fossa and condyle of up to 1mm ᕤ Upper molar distal rotation ᕥ Intrusion of the upper molars and counter clockwise rotation of the mandible ᕦ Lower molar extrusion to hold the Class II correction ᕧ Condyle and glenoid fossa growth in the growing patient Although 18x25S wires can be used with the TFBC, this author prefers a 19x25S in the .022 slot for greater control of incisor torque in combination with the MBT bracket Rx, which has increased upper incisor torque and decreased lower incisor torque values from a standard Roth Rx. (Fig .12) This combination is advantageous to mitigate the effects of Class II mechanics, which decrease 7 Mechanisms The Twin Force Bite Corrector utilizes seven mechanisms to correct the Class II dental occlu-sions and can achieve skeletal changes in the growing patient. The mechanisms of treatment include: ᕡ Maxillary arch distalization of up to 1.5mm www.orthodontics.com Spring 2022 15
Journal of the American Orthodontic Society Spring 2022: Page 15