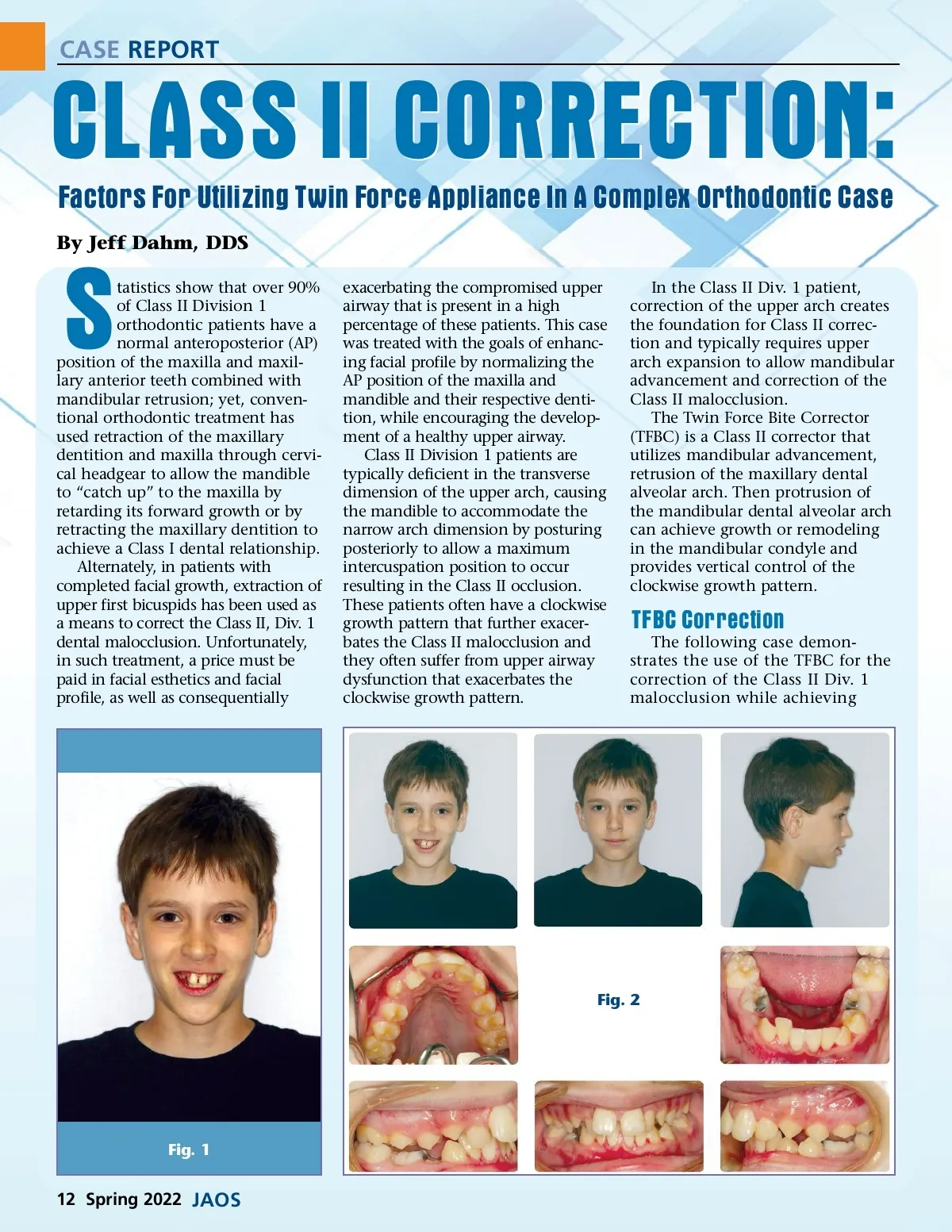
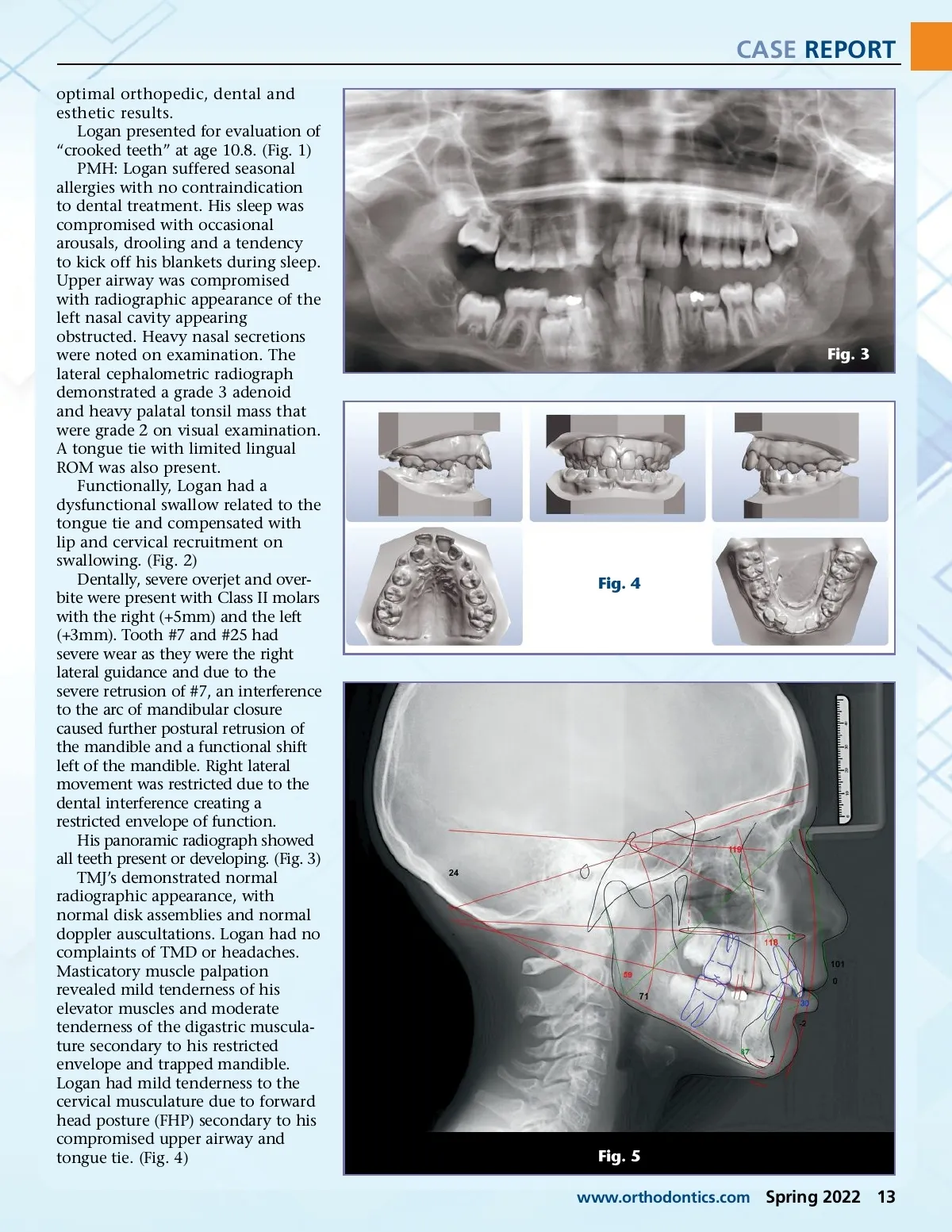
CASE REPORT optimal orthopedic, dental and esthetic results. Logan presented for evaluation of “crooked teeth” at age 10.8. (Fig. 1) PMH: Logan suffered seasonal allergies with no contraindication to dental treatment. His sleep was compromised with occasional arousals, drooling and a tendency to kick off his blankets during sleep. Upper airway was compromised with radiographic appearance of the left nasal cavity appearing obstructed. Heavy nasal secretions were noted on examination. The lateral cephalometric radiograph demonstrated a grade 3 adenoid and heavy palatal tonsil mass that were grade 2 on visual examination. A tongue tie with limited lingual ROM was also present. Functionally, Logan had a dysfunctional swallow related to the tongue tie and compensated with lip and cervical recruitment on swallowing. (Fig. 2) Dentally, severe overjet and over-bite were present with Class II molars with the right (+5mm) and the left (+3mm). Tooth #7 and #25 had severe wear as they were the right lateral guidance and due to the severe retrusion of #7, an interference to the arc of mandibular closure caused further postural retrusion of the mandible and a functional shift left of the mandible. Right lateral movement was restricted due to the dental interference creating a restricted envelope of function. His panoramic radiograph showed all teeth present or developing. (Fig. 3) TMJ’s demonstrated normal radiographic appearance, with normal disk assemblies and normal doppler auscultations. Logan had no complaints of TMD or headaches. Masticatory muscle palpation revealed mild tenderness of his elevator muscles and moderate tenderness of the digastric muscula-ture secondary to his restricted envelope and trapped mandible. Logan had mild tenderness to the cervical musculature due to forward head posture (FHP) secondary to his compromised upper airway and tongue tie. (Fig. 4) Fig. 3 Fig. 4 Fig. 5 www.orthodontics.com Spring 2022 13
Journal of the American Orthodontic Society Spring 2022: Page 13