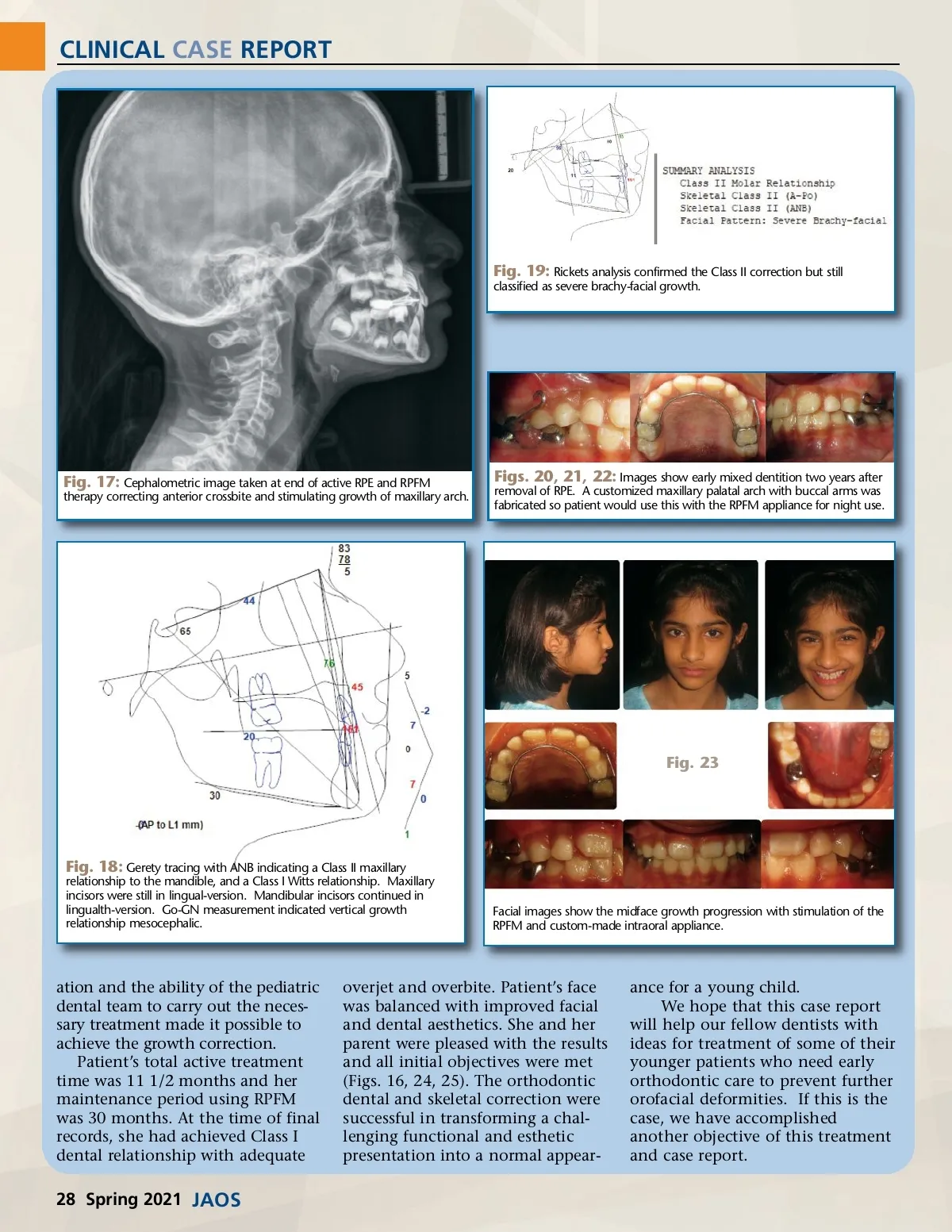
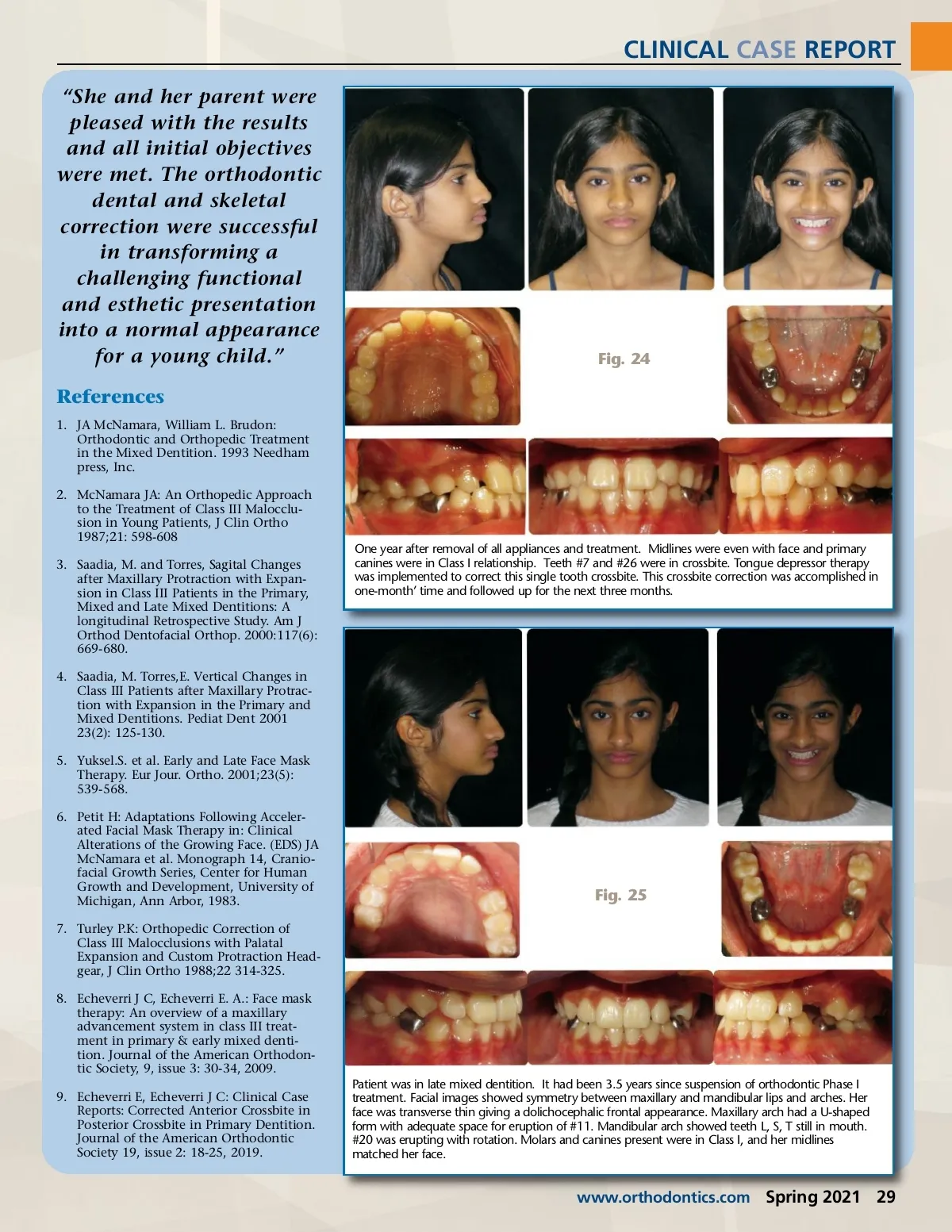
CLINICAL CASE REPORT Fig. 19: Rickets analysis confirmed the Class II correction but still classified as severe brachy-facial growth. Fig. 17: Cephalometric image taken at end of active RPE and RPFM therapy correcting anterior crossbite and stimulating growth of maxillary arch. Figs. 20, 21, 22: Images show early mixed dentition two years after removal of RPE. A customized maxillary palatal arch with buccal arms was fabricated so patient would use this with the RPFM appliance for night use. Fig. 23 Fig. 18: Gerety tracing with ANB indicating a Class II maxillary relationship to the mandible, and a Class I Witts relationship. Maxillary incisors were still in lingual-version. Mandibular incisors continued in lingualth-version. Go-GN measurement indicated vertical growth relationship mesocephalic. Facial images show the midface growth progression with stimulation of the RPFM and custom-made intraoral appliance. ation and the ability of the pediatric dental team to carry out the neces-sary treatment made it possible to achieve the growth correction. Patient’s total active treatment time was 11 1/2 months and her maintenance period using RPFM was 30 months. At the time of final records, she had achieved Class I dental relationship with adequate overjet and overbite. Patient’s face was balanced with improved facial and dental aesthetics. She and her parent were pleased with the results and all initial objectives were met (Figs. 16, 24, 25). The orthodontic dental and skeletal correction were successful in transforming a chal-lenging functional and esthetic presentation into a normal appear-ance for a young child. We hope that this case report will help our fellow dentists with ideas for treatment of some of their younger patients who need early orthodontic care to prevent further orofacial deformities. If this is the case, we have accomplished another objective of this treatment and case report. 28 Spring 2021 JAOS
Journal of the American Orthodontic Society Spring 2021: Page 28