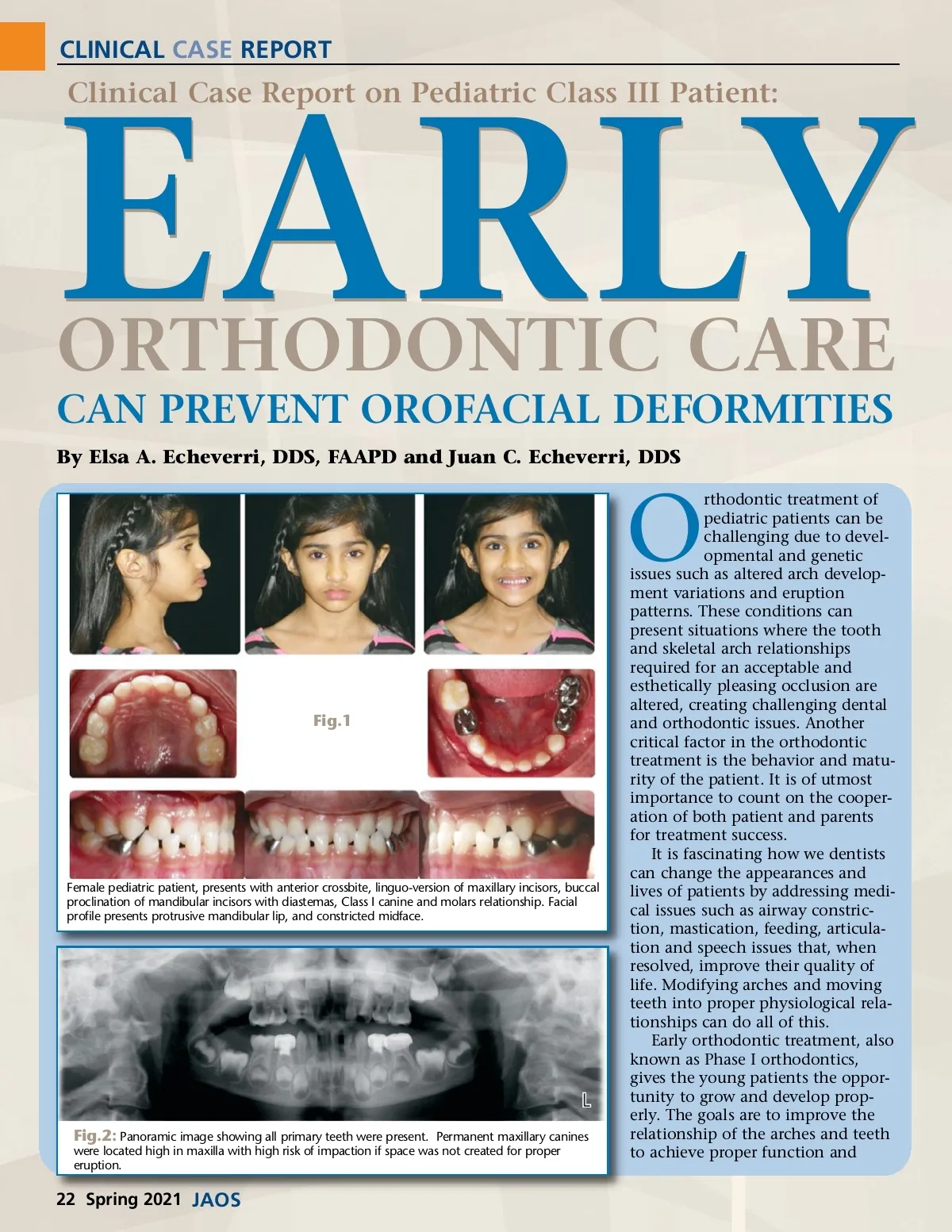
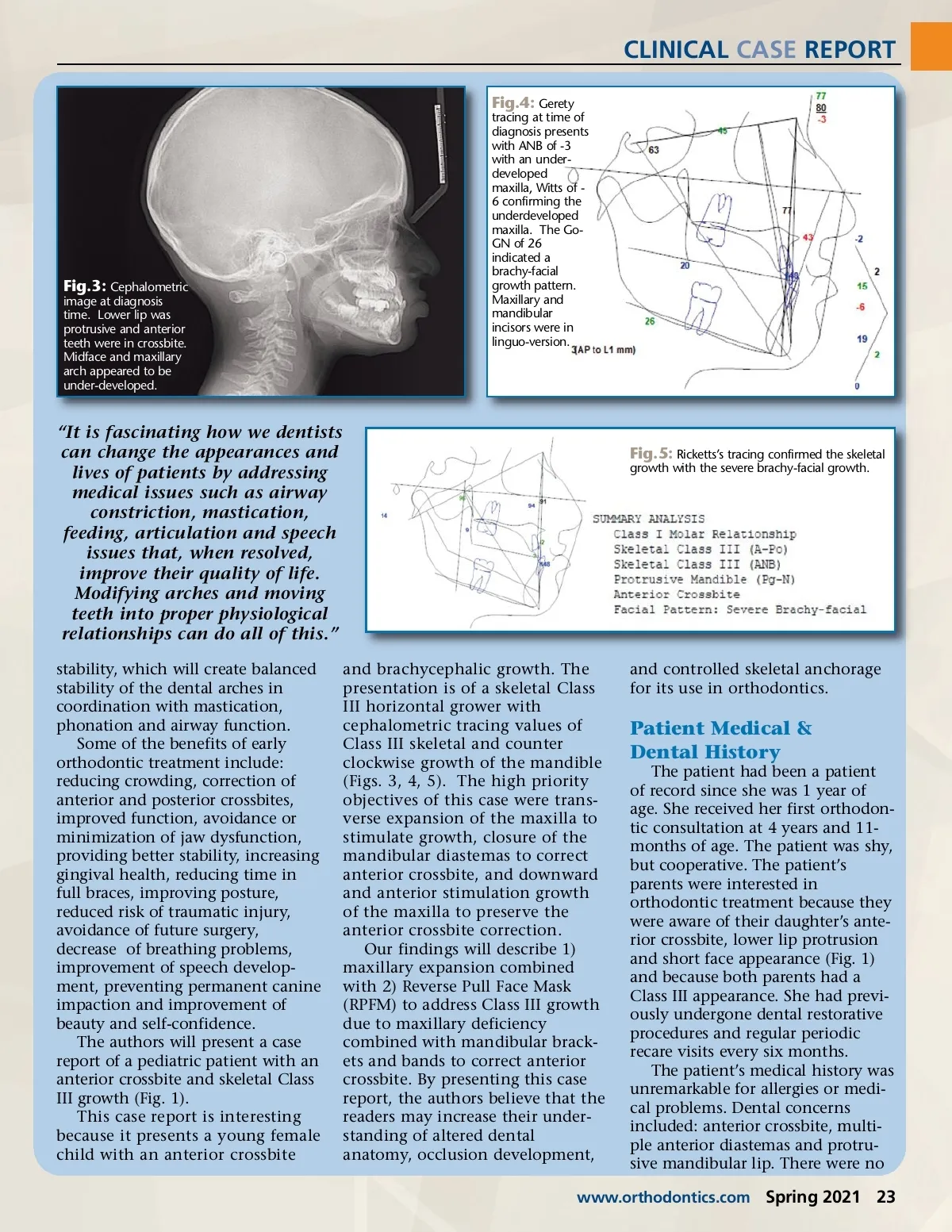
CLINICAL CASE REPORT Fig.4: Gerety tracing at time of diagnosis presents with ANB of -3 with an under-developed maxilla, Witts of -6 confirming the underdeveloped maxilla. The Go-GN of 26 indicated a brachy-facial growth pattern. Maxillary and mandibular incisors were in linguo-version. Fig.3: Cephalometric image at diagnosis time. Lower lip was protrusive and anterior teeth were in crossbite. Midface and maxillary arch appeared to be under-developed. “It is fascinating how we dentists can change the appearances and lives of patients by addressing medical issues such as airway constriction, mastication, feeding, articulation and speech issues that, when resolved, improve their quality of life. Modifying arches and moving teeth into proper physiological relationships can do all of this.” stability, which will create balanced stability of the dental arches in coordination with mastication, phonation and airway function. Some of the benefits of early orthodontic treatment include: reducing crowding, correction of anterior and posterior crossbites, improved function, avoidance or minimization of jaw dysfunction, providing better stability, increasing gingival health, reducing time in full braces, improving posture, reduced risk of traumatic injury, avoidance of future surgery, decrease of breathing problems, improvement of speech develop-ment, preventing permanent canine impaction and improvement of beauty and self-confidence. The authors will present a case report of a pediatric patient with an anterior crossbite and skeletal Class III growth (Fig. 1). This case report is interesting because it presents a young female child with an anterior crossbite and brachycephalic growth. The presentation is of a skeletal Class III horizontal grower with cephalometric tracing values of Class III skeletal and counter clockwise growth of the mandible (Figs. 3, 4, 5). The high priority objectives of this case were trans-verse expansion of the maxilla to stimulate growth, closure of the mandibular diastemas to correct anterior crossbite, and downward and anterior stimulation growth of the maxilla to preserve the anterior crossbite correction. Our findings will describe 1) maxillary expansion combined with 2) Reverse Pull Face Mask (RPFM) to address Class III growth due to maxillary deficiency combined with mandibular brack-ets and bands to correct anterior crossbite. By presenting this case report, the authors believe that the readers may increase their under-standing of altered dental anatomy, occlusion development, Fig.5: Ricketts’s tracing confirmed the skeletal growth with the severe brachy-facial growth. and controlled skeletal anchorage for its use in orthodontics. Patient Medical & Dental History The patient had been a patient of record since she was 1 year of age. She received her first orthodon-tic consultation at 4 years and 11-months of age. The patient was shy, but cooperative. The patient’s parents were interested in orthodontic treatment because they were aware of their daughter’s ante-rior crossbite, lower lip protrusion and short face appearance (Fig. 1) and because both parents had a Class III appearance. She had previ-ously undergone dental restorative procedures and regular periodic recare visits every six months. The patient’s medical history was unremarkable for allergies or medi-cal problems. Dental concerns included: anterior crossbite, multi-ple anterior diastemas and protru-sive mandibular lip. There were no www.orthodontics.com Spring 2021 23
Journal of the American Orthodontic Society Spring 2021: Page 23