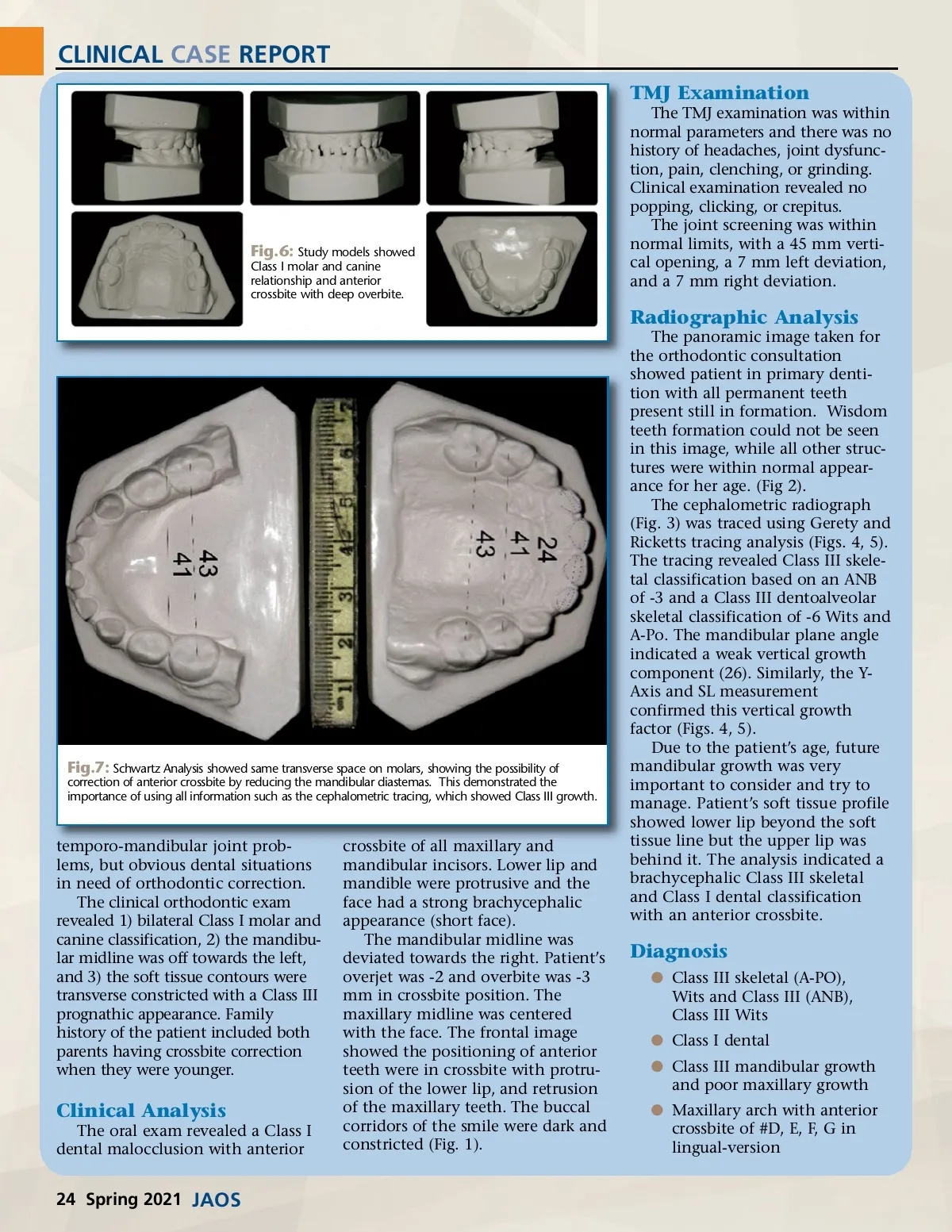
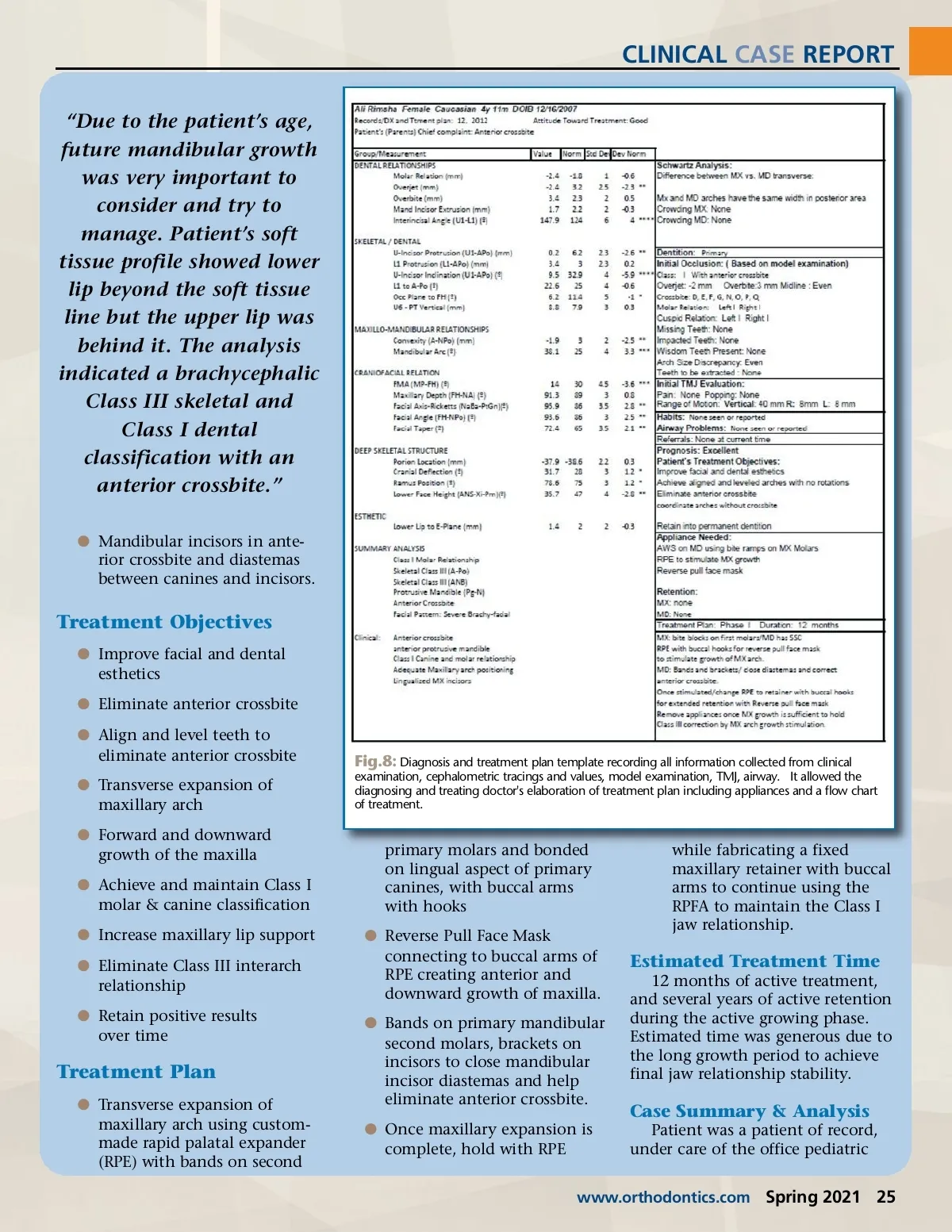
CLINICAL CASE REPORT TMJ Examination The TMJ examination was within normal parameters and there was no history of headaches, joint dysfunc-tion, pain, clenching, or grinding. Clinical examination revealed no popping, clicking, or crepitus. The joint screening was within normal limits, with a 45 mm verti-cal opening, a 7 mm left deviation, and a 7 mm right deviation. Fig.6: Study models showed Class I molar and canine relationship and anterior crossbite with deep overbite. Radiographic Analysis The panoramic image taken for the orthodontic consultation showed patient in primary denti-tion with all permanent teeth present still in formation. Wisdom teeth formation could not be seen in this image, while all other struc-tures were within normal appear-ance for her age. (Fig 2). The cephalometric radiograph (Fig. 3) was traced using Gerety and Ricketts tracing analysis (Figs. 4, 5). The tracing revealed Class III skele-tal classification based on an ANB of -3 and a Class III dentoalveolar skeletal classification of -6 Wits and A-Po. The mandibular plane angle indicated a weak vertical growth component (26). Similarly, the Y-Axis and SL measurement confirmed this vertical growth factor (Figs. 4, 5). Due to the patient’s age, future mandibular growth was very important to consider and try to manage. Patient’s soft tissue profile showed lower lip beyond the soft tissue line but the upper lip was behind it. The analysis indicated a brachycephalic Class III skeletal and Class I dental classification with an anterior crossbite. Fig.7: Schwartz Analysis showed same transverse space on molars, showing the possibility of correction of anterior crossbite by reducing the mandibular diastemas. This demonstrated the importance of using all information such as the cephalometric tracing, which showed Class III growth. temporo-mandibular joint prob-lems, but obvious dental situations in need of orthodontic correction. The clinical orthodontic exam revealed 1) bilateral Class I molar and canine classification, 2) the mandibu-lar midline was off towards the left, and 3) the soft tissue contours were transverse constricted with a Class III prognathic appearance. Family history of the patient included both parents having crossbite correction when they were younger. crossbite of all maxillary and mandibular incisors. Lower lip and mandible were protrusive and the face had a strong brachycephalic appearance (short face). The mandibular midline was deviated towards the right. Patient’s overjet was -2 and overbite was -3 mm in crossbite position. The maxillary midline was centered with the face. The frontal image showed the positioning of anterior teeth were in crossbite with protru-sion of the lower lip, and retrusion of the maxillary teeth. The buccal corridors of the smile were dark and constricted (Fig. 1). Diagnosis b Class III skeletal (A-PO), Wits and Class III (ANB), Class III Wits b Class I dental b Class III mandibular growth and poor maxillary growth b Maxillary arch with anterior crossbite of #D, E, F, G in lingual-version Clinical Analysis The oral exam revealed a Class I dental malocclusion with anterior 24 Spring 2021 JAOS
Journal of the American Orthodontic Society Spring 2021: Page 24