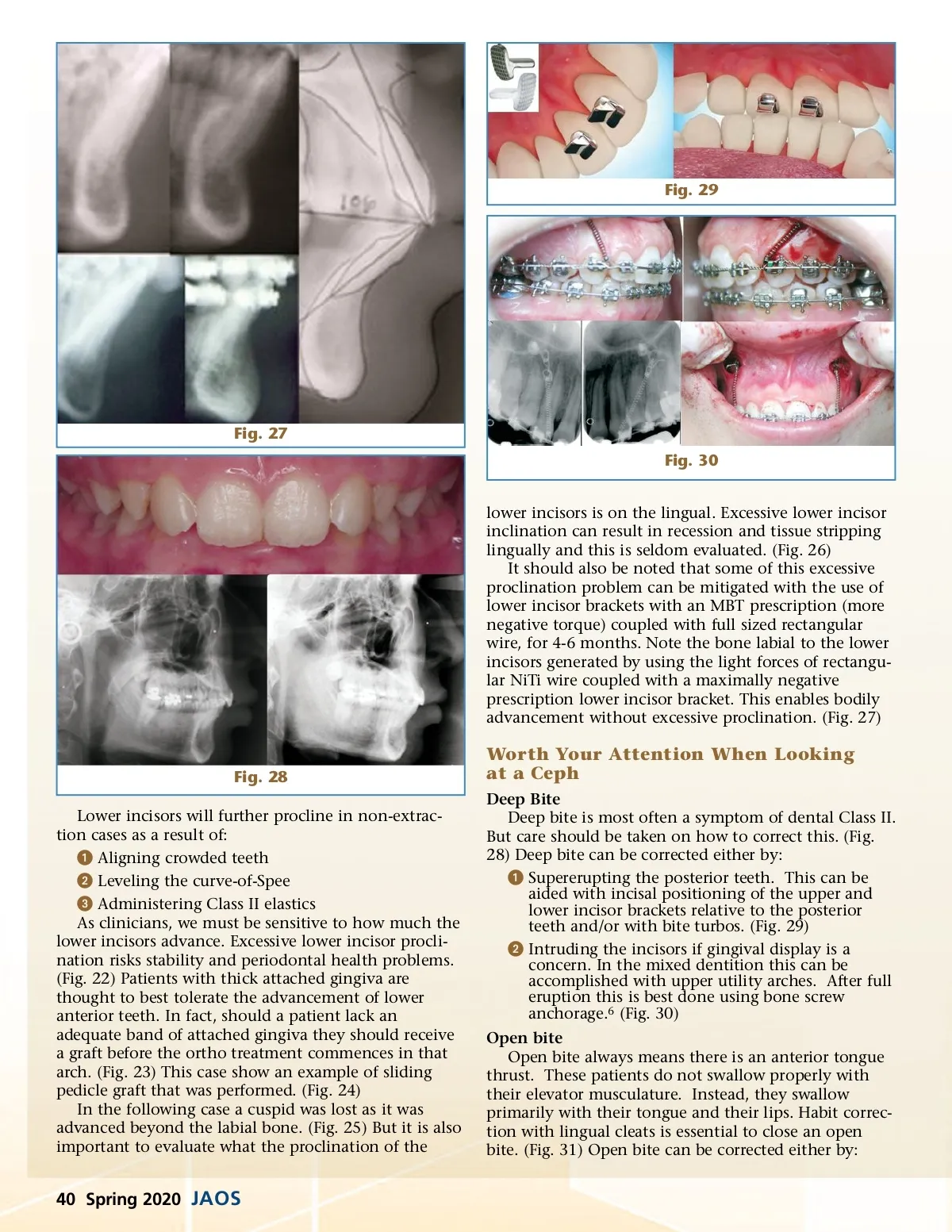
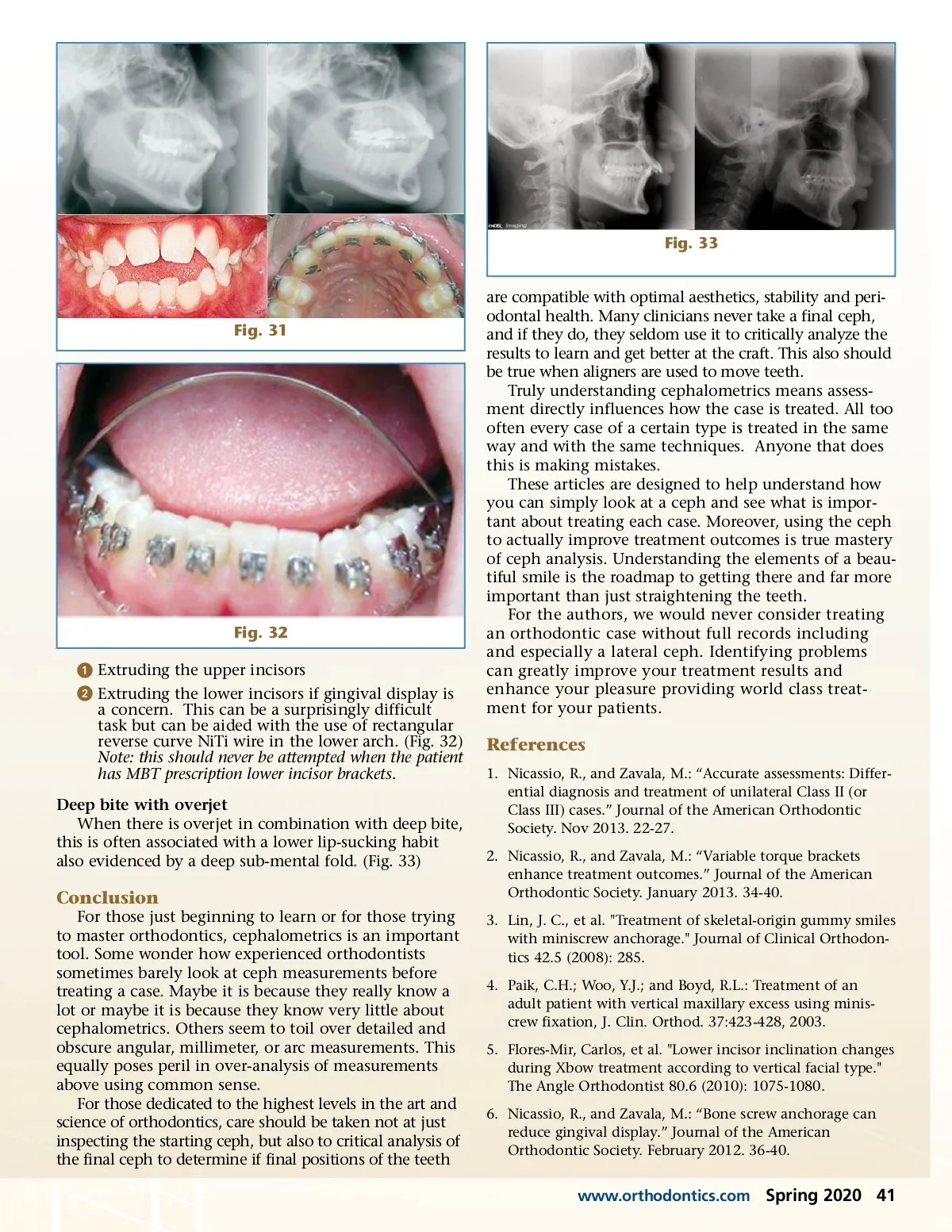
Fig. 29 Fig. 27 Fig. 30 lower incisors is on the lingual. Excessive lower incisor inclination can result in recession and tissue stripping lingually and this is seldom evaluated. (Fig. 26) It should also be noted that some of this excessive proclination problem can be mitigated with the use of lower incisor brackets with an MBT prescription (more negative torque) coupled with full sized rectangular wire, for 4-6 months. Note the bone labial to the lower incisors generated by using the light forces of rectangu-lar NiTi wire coupled with a maximally negative prescription lower incisor bracket. This enables bodily advancement without excessive proclination. (Fig. 27) Fig. 28 Lower incisors will further procline in non-extrac-tion cases as a result of: ᕡ Aligning crowded teeth ᕢ Leveling the curve-of-Spee ᕣ Administering Class II elastics As clinicians, we must be sensitive to how much the lower incisors advance. Excessive lower incisor procli-nation risks stability and periodontal health problems. (Fig. 22) Patients with thick attached gingiva are thought to best tolerate the advancement of lower anterior teeth. In fact, should a patient lack an adequate band of attached gingiva they should receive a graft before the ortho treatment commences in that arch. (Fig. 23) This case show an example of sliding pedicle graft that was performed. (Fig. 24) In the following case a cuspid was lost as it was advanced beyond the labial bone. (Fig. 25) But it is also important to evaluate what the proclination of the Worth Your Attention When Looking at a Ceph Deep Bite Deep bite is most often a symptom of dental Class II. But care should be taken on how to correct this. (Fig. 28) Deep bite can be corrected either by: ᕡ Supererupting the posterior teeth. This can be aided with incisal positioning of the upper and lower incisor brackets relative to the posterior teeth and/or with bite turbos. (Fig. 29) ᕢ Intruding the incisors if gingival display is a concern. In the mixed dentition this can be accomplished with upper utility arches. After full eruption this is best done using bone screw anchorage. 6 (Fig. 30) Open bite Open bite always means there is an anterior tongue thrust. These patients do not swallow properly with their elevator musculature. Instead, they swallow primarily with their tongue and their lips. Habit correc-tion with lingual cleats is essential to close an open bite. (Fig. 31) Open bite can be corrected either by: 40 Spring 2020 JAOS
Journal of the American Orthodontic Society Spring 2020: Page 40