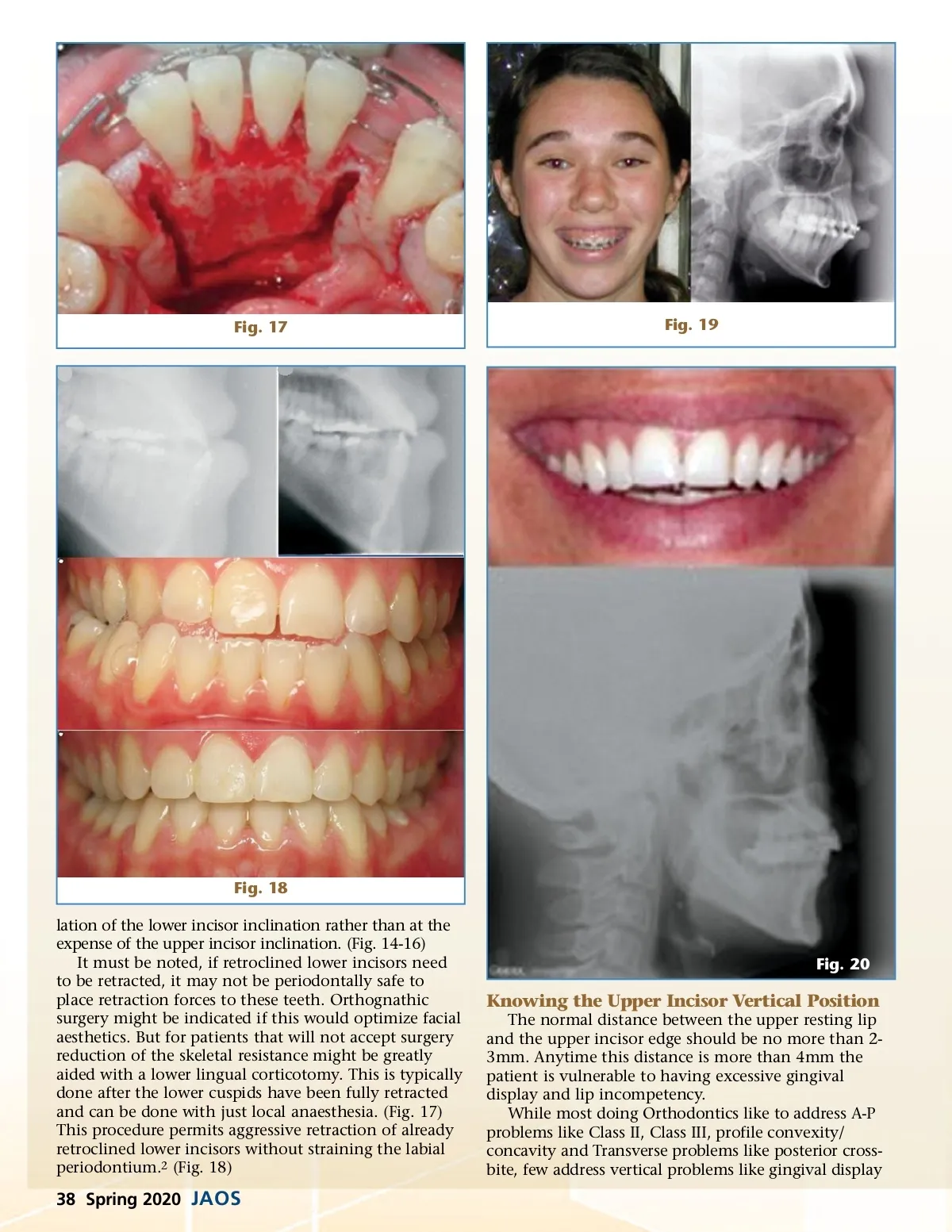
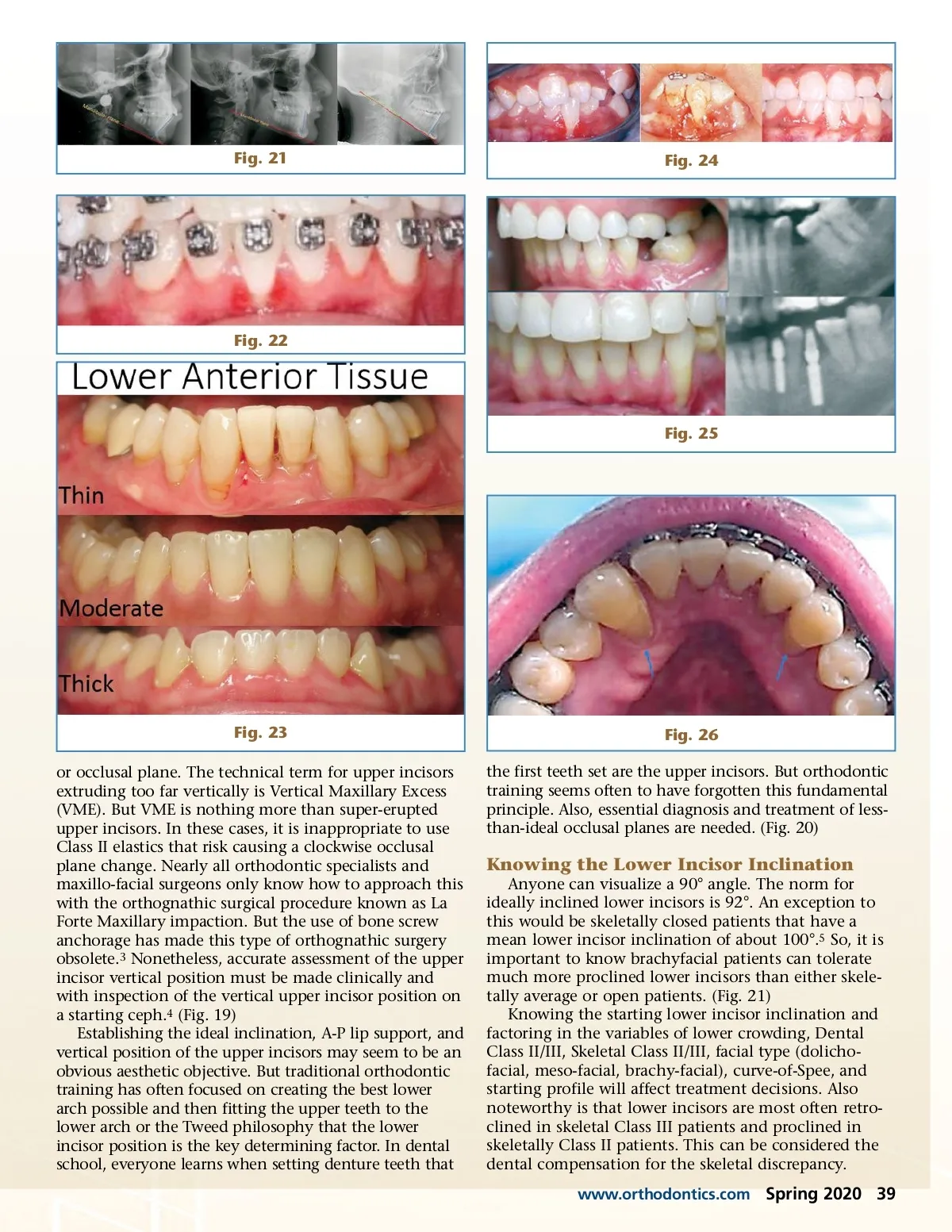
Fig. 21 Fig. 24 Fig. 22 Fig. 25 Fig. 23 or occlusal plane. The technical term for upper incisors extruding too far vertically is Vertical Maxillary Excess (VME). But VME is nothing more than super-erupted upper incisors. In these cases, it is inappropriate to use Class II elastics that risk causing a clockwise occlusal plane change. Nearly all orthodontic specialists and maxillo-facial surgeons only know how to approach this with the orthognathic surgical procedure known as La Forte Maxillary impaction. But the use of bone screw anchorage has made this type of orthognathic surgery obsolete. 3 Nonetheless, accurate assessment of the upper incisor vertical position must be made clinically and with inspection of the vertical upper incisor position on a starting ceph. 4 (Fig. 19) Establishing the ideal inclination, A-P lip support, and vertical position of the upper incisors may seem to be an obvious aesthetic objective. But traditional orthodontic training has often focused on creating the best lower arch possible and then fitting the upper teeth to the lower arch or the Tweed philosophy that the lower incisor position is the key determining factor. In dental school, everyone learns when setting denture teeth that Fig. 26 the first teeth set are the upper incisors. But orthodontic training seems often to have forgotten this fundamental principle. Also, essential diagnosis and treatment of less-than-ideal occlusal planes are needed. (Fig. 20) Knowing the Lower Incisor Inclination Anyone can visualize a 90° angle. The norm for ideally inclined lower incisors is 92°. An exception to this would be skeletally closed patients that have a mean lower incisor inclination of about 100°. 5 So, it is important to know brachyfacial patients can tolerate much more proclined lower incisors than either skele-tally average or open patients. (Fig. 21) Knowing the starting lower incisor inclination and factoring in the variables of lower crowding, Dental Class II/III, Skeletal Class II/III, facial type (dolicho-facial, meso-facial, brachy-facial), curve-of-Spee, and starting profile will affect treatment decisions. Also noteworthy is that lower incisors are most often retro-clined in skeletal Class III patients and proclined in skeletally Class II patients. This can be considered the dental compensation for the skeletal discrepancy. www.orthodontics.com Spring 2020 39
Journal of the American Orthodontic Society Spring 2020: Page 39