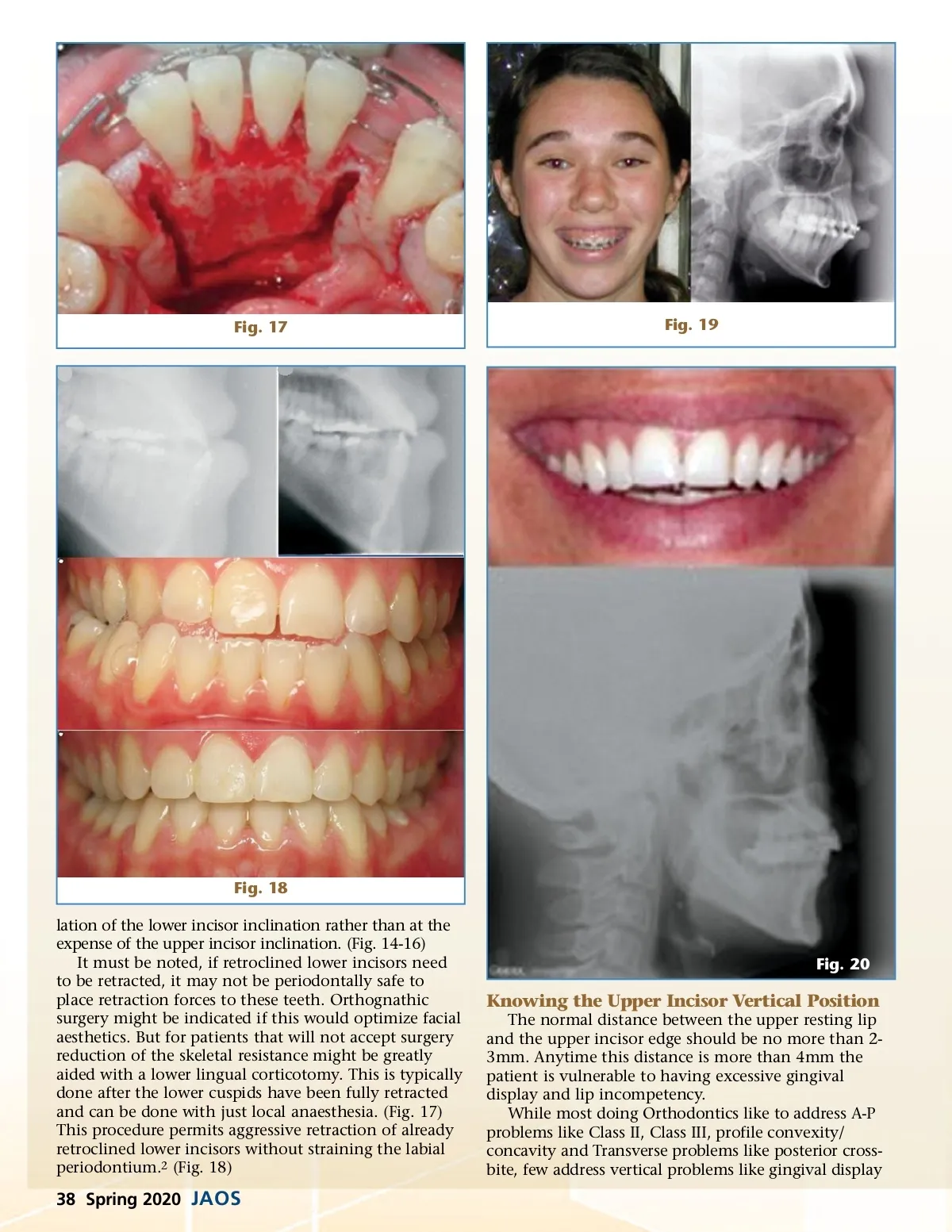
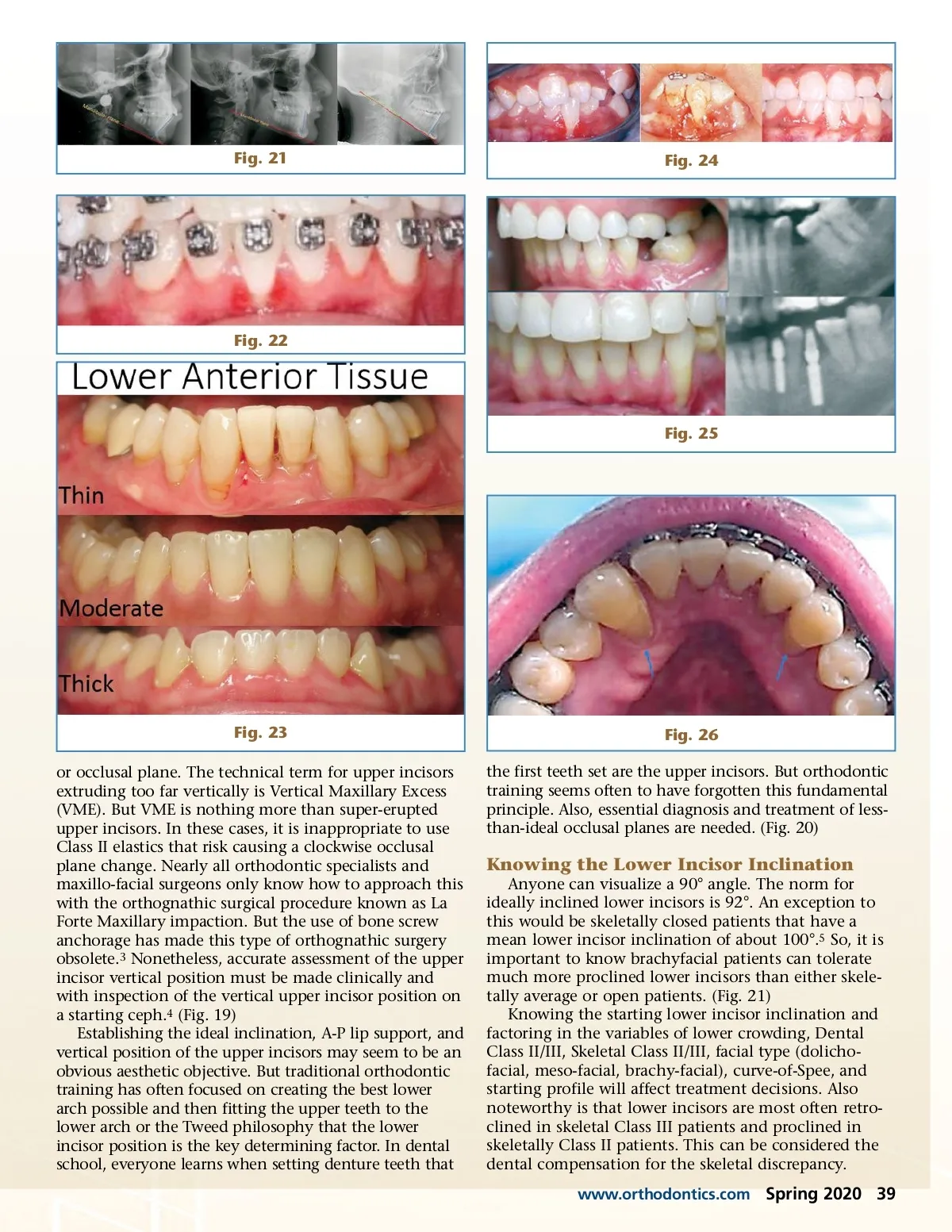
Fig. 17 Fig. 19 Fig. 18 lation of the lower incisor inclination rather than at the expense of the upper incisor inclination. (Fig. 14-16) It must be noted, if retroclined lower incisors need to be retracted, it may not be periodontally safe to place retraction forces to these teeth. Orthognathic surgery might be indicated if this would optimize facial aesthetics. But for patients that will not accept surgery reduction of the skeletal resistance might be greatly aided with a lower lingual corticotomy. This is typically done after the lower cuspids have been fully retracted and can be done with just local anaesthesia. (Fig. 17) This procedure permits aggressive retraction of already retroclined lower incisors without straining the labial periodontium. 2 (Fig. 18) Fig. 20 Knowing the Upper Incisor Vertical Position The normal distance between the upper resting lip and the upper incisor edge should be no more than 2-3mm. Anytime this distance is more than 4mm the patient is vulnerable to having excessive gingival display and lip incompetency. While most doing Orthodontics like to address A-P problems like Class II, Class III, profile convexity/ concavity and Transverse problems like posterior cross-bite, few address vertical problems like gingival display 38 Spring 2020 JAOS
Journal of the American Orthodontic Society Spring 2020: Page 38