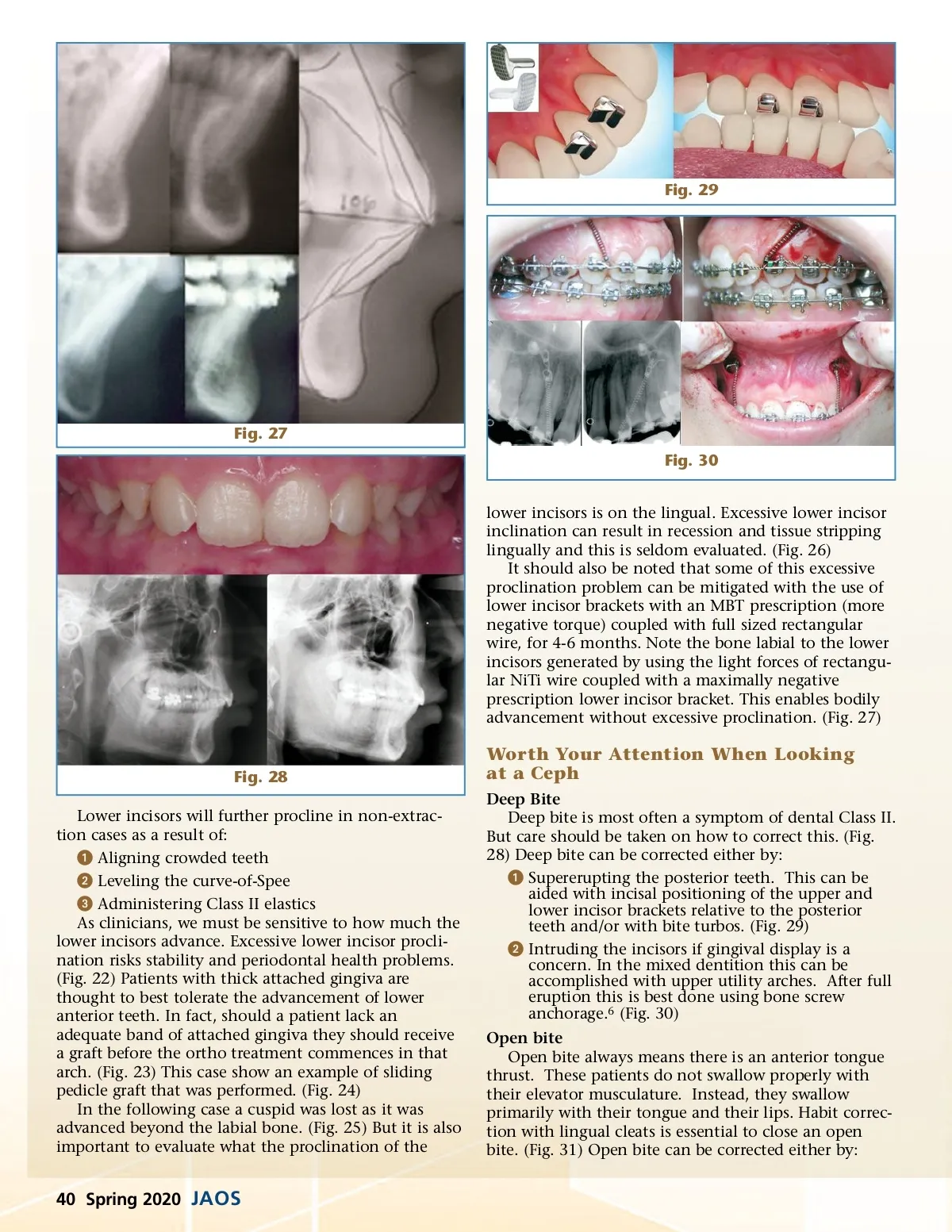
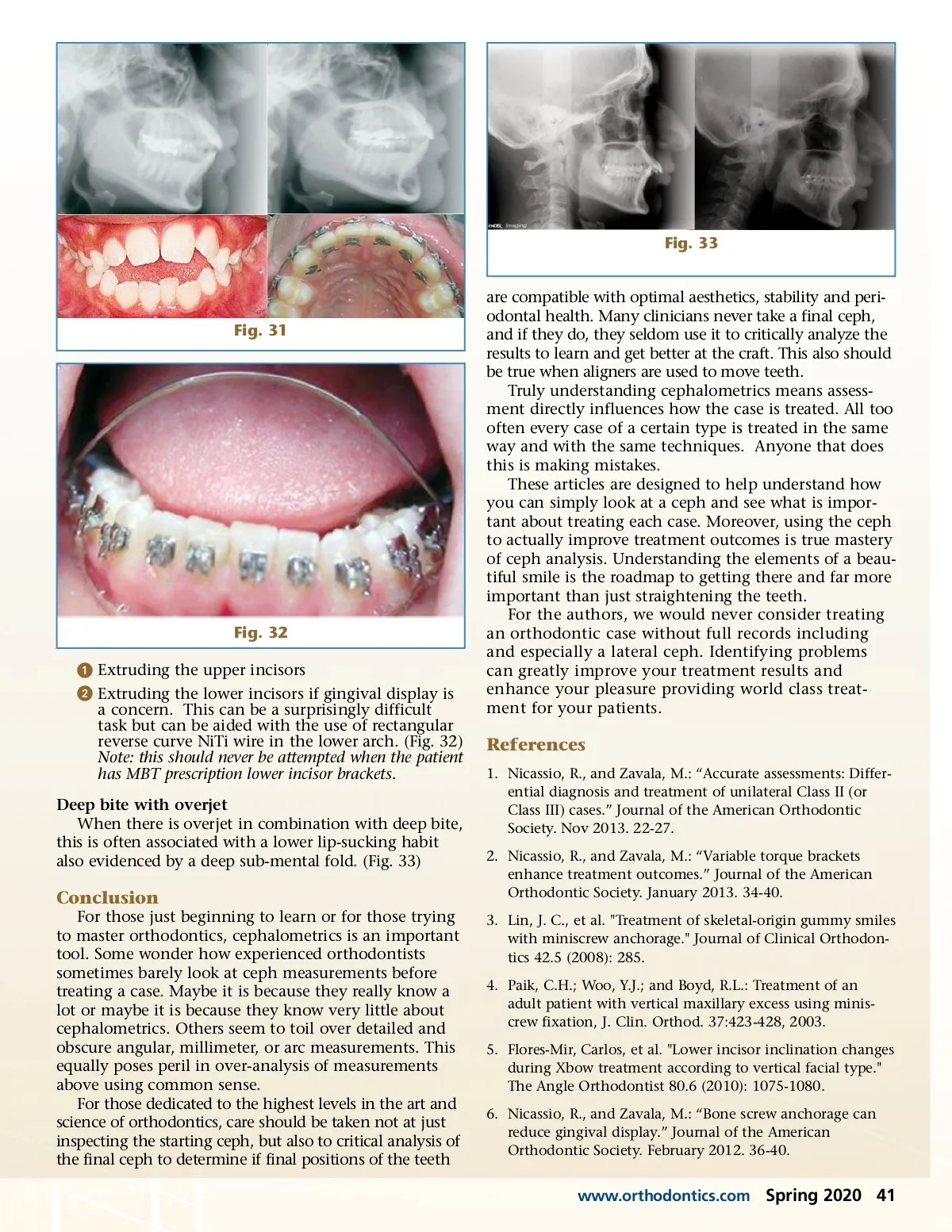
Fig. 33 are compatible with optimal aesthetics, stability and peri-odontal health. Many clinicians never take a final ceph, and if they do, they seldom use it to critically analyze the results to learn and get better at the craft. This also should be true when aligners are used to move teeth. Truly understanding cephalometrics means assess-ment directly influences how the case is treated. All too often every case of a certain type is treated in the same way and with the same techniques. Anyone that does this is making mistakes. These articles are designed to help understand how you can simply look at a ceph and see what is impor-tant about treating each case. Moreover, using the ceph to actually improve treatment outcomes is true mastery of ceph analysis. Understanding the elements of a beau-tiful smile is the roadmap to getting there and far more important than just straightening the teeth. For the authors, we would never consider treating an orthodontic case without full records including and especially a lateral ceph. Identifying problems can greatly improve your treatment results and enhance your pleasure providing world class treat-ment for your patients. Fig. 31 Fig. 32 ᕡ Extruding the upper incisors ᕢ Extruding the lower incisors if gingival display is a concern. This can be a surprisingly difficult task but can be aided with the use of rectangular reverse curve NiTi wire in the lower arch. (Fig. 32) Note: this should never be attempted when the patient has MBT prescription lower incisor brackets. Deep bite with overjet When there is overjet in combination with deep bite, this is often associated with a lower lip-sucking habit also evidenced by a deep sub-mental fold. (Fig. 33) References 1. Nicassio, R., and Zavala, M.: “Accurate assessments: Differ-ential diagnosis and treatment of unilateral Class II (or Class III) cases.” Journal of the American Orthodontic Society. Nov 2013. 22-27. 2. Nicassio, R., and Zavala, M.: “Variable torque brackets enhance treatment outcomes.” Journal of the American Orthodontic Society. January 2013. 34-40. 3. Lin, J. C., et al. "Treatment of skeletal-origin gummy smiles with miniscrew anchorage." Journal of Clinical Orthodon-tics 42.5 (2008): 285. 4. Paik, C.H.; Woo, Y.J.; and Boyd, R.L.: Treatment of an adult patient with vertical maxillary excess using minis-crew fixation, J. Clin. Orthod. 37:423-428, 2003. 5. Flores-Mir, Carlos, et al. "Lower incisor inclination changes during Xbow treatment according to vertical facial type." The Angle Orthodontist 80.6 (2010): 1075-1080. 6. Nicassio, R., and Zavala, M.: “Bone screw anchorage can reduce gingival display.” Journal of the American Orthodontic Society. February 2012. 36-40. Conclusion For those just beginning to learn or for those trying to master orthodontics, cephalometrics is an important tool. Some wonder how experienced orthodontists sometimes barely look at ceph measurements before treating a case. Maybe it is because they really know a lot or maybe it is because they know very little about cephalometrics. Others seem to toil over detailed and obscure angular, millimeter, or arc measurements. This equally poses peril in over-analysis of measurements above using common sense. For those dedicated to the highest levels in the art and science of orthodontics, care should be taken not at just inspecting the starting ceph, but also to critical analysis of the final ceph to determine if final positions of the teeth www.orthodontics.com Spring 2020 41
Journal of the American Orthodontic Society Spring 2020: Page 41