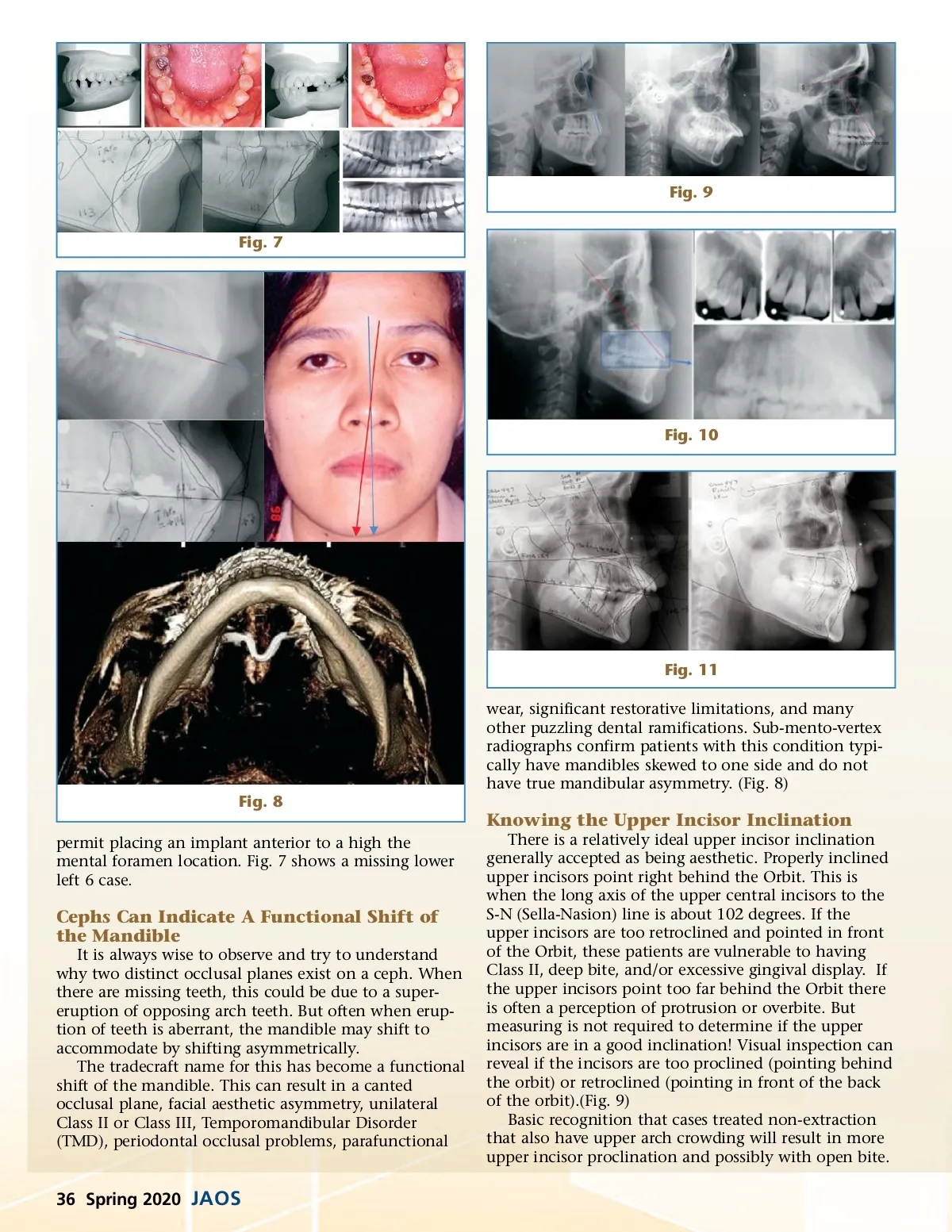
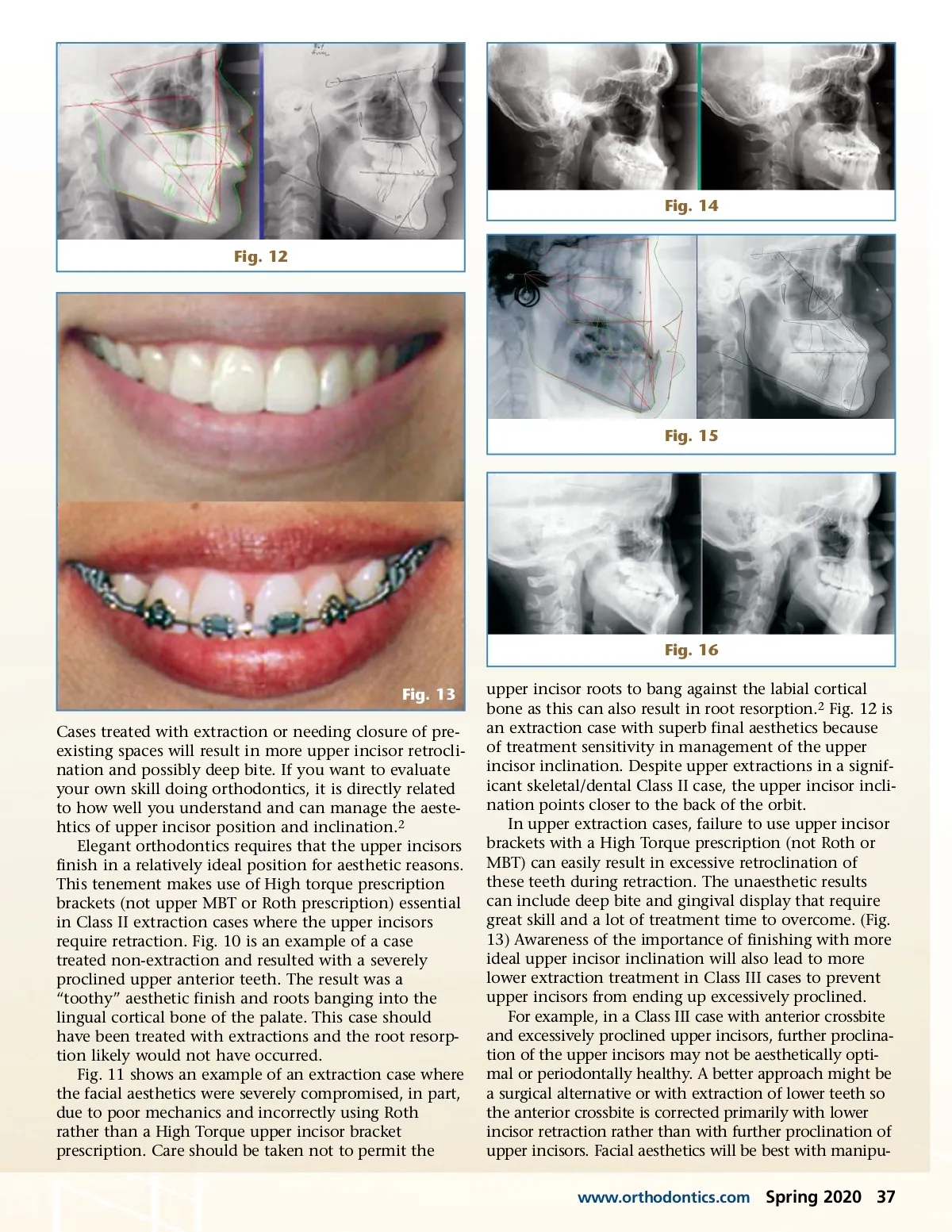
Fig. 9 Fig. 7 Fig. 10 Fig. 11 wear, significant restorative limitations, and many other puzzling dental ramifications. Sub-mento-vertex radiographs confirm patients with this condition typi-cally have mandibles skewed to one side and do not have true mandibular asymmetry. (Fig. 8) Fig. 8 Knowing the Upper Incisor Inclination permit placing an implant anterior to a high the mental foramen location. Fig. 7 shows a missing lower left 6 case. There is a relatively ideal upper incisor inclination generally accepted as being aesthetic. Properly inclined upper incisors point right behind the Orbit. This is when the long axis of the upper central incisors to the S-N (Sella-Nasion) line is about 102 degrees. If the upper incisors are too retroclined and pointed in front of the Orbit, these patients are vulnerable to having Class II, deep bite, and/or excessive gingival display. If the upper incisors point too far behind the Orbit there is often a perception of protrusion or overbite. But measuring is not required to determine if the upper incisors are in a good inclination! Visual inspection can reveal if the incisors are too proclined (pointing behind the orbit) or retroclined (pointing in front of the back of the orbit).(Fig. 9) Basic recognition that cases treated non-extraction that also have upper arch crowding will result in more upper incisor proclination and possibly with open bite. Cephs Can Indicate A Functional Shift of the Mandible It is always wise to observe and try to understand why two distinct occlusal planes exist on a ceph. When there are missing teeth, this could be due to a super-eruption of opposing arch teeth. But often when erup-tion of teeth is aberrant, the mandible may shift to accommodate by shifting asymmetrically. The tradecraft name for this has become a functional shift of the mandible. This can result in a canted occlusal plane, facial aesthetic asymmetry, unilateral Class II or Class III, Temporomandibular Disorder (TMD), periodontal occlusal problems, parafunctional 36 Spring 2020 JAOS
Journal of the American Orthodontic Society Spring 2020: Page 36