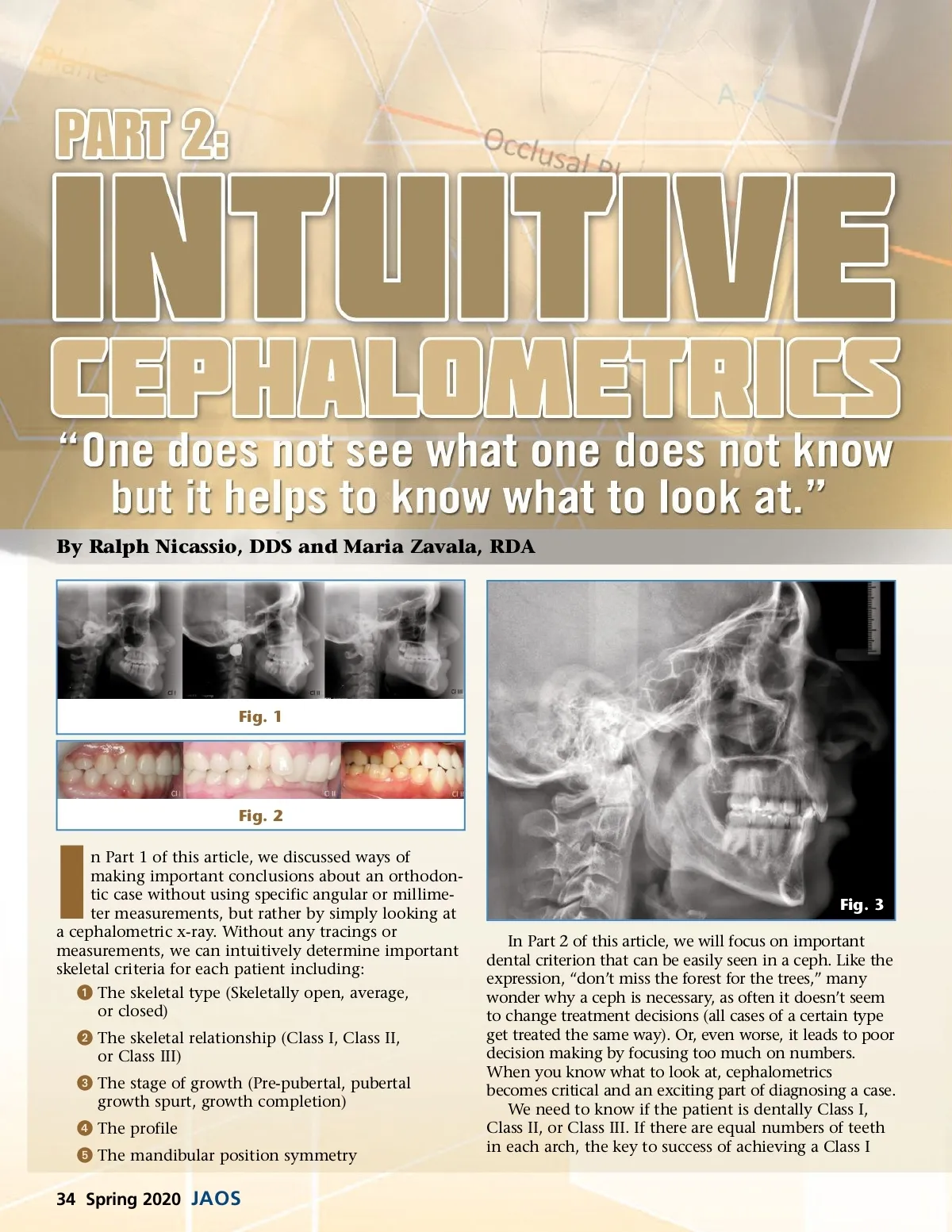
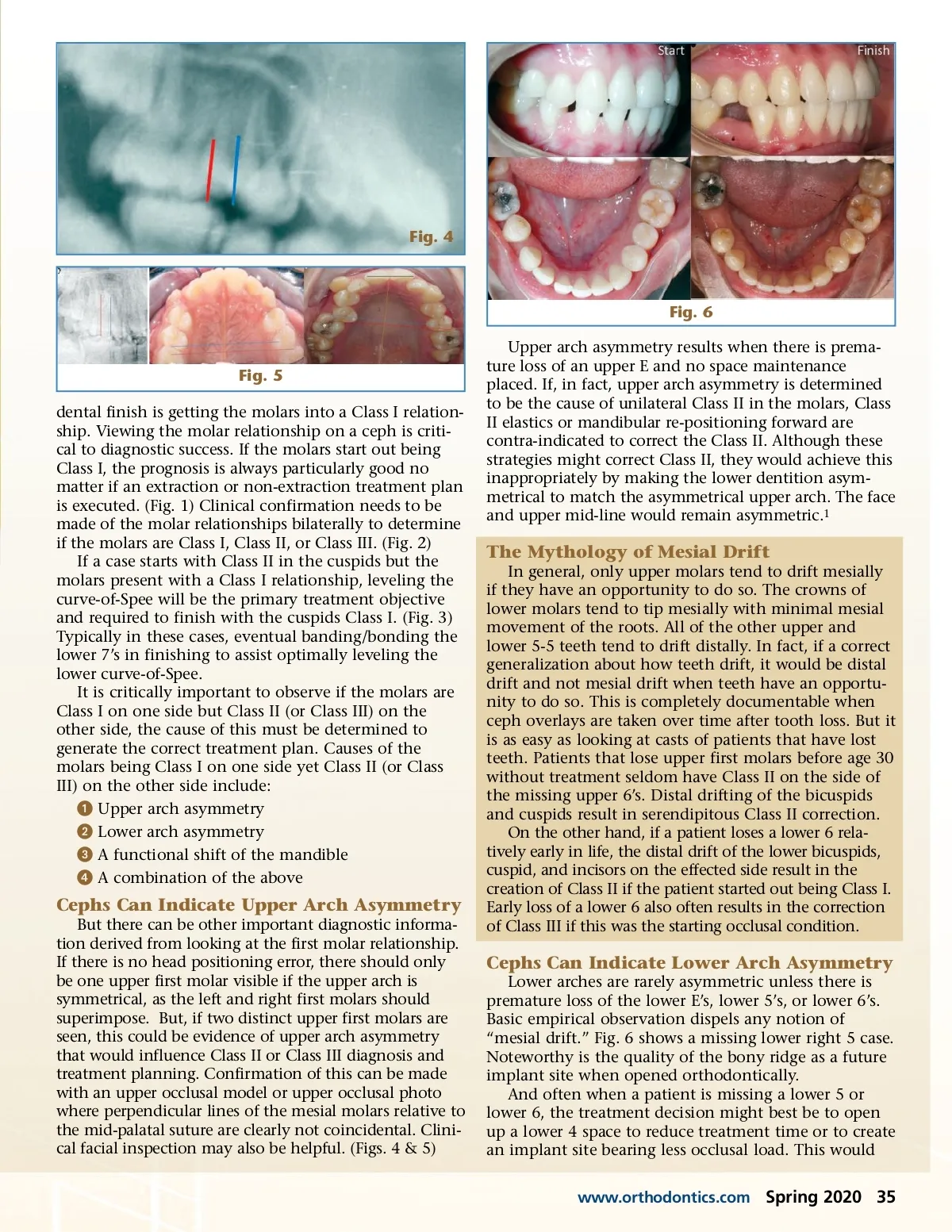
Fig. 4 Fig. 6 Upper arch asymmetry results when there is prema-ture loss of an upper E and no space maintenance placed. If, in fact, upper arch asymmetry is determined to be the cause of unilateral Class II in the molars, Class II elastics or mandibular re-positioning forward are contra-indicated to correct the Class II. Although these strategies might correct Class II, they would achieve this inappropriately by making the lower dentition asym-metrical to match the asymmetrical upper arch. The face and upper mid-line would remain asymmetric. 1 Fig. 5 dental finish is getting the molars into a Class I relation-ship. Viewing the molar relationship on a ceph is criti-cal to diagnostic success. If the molars start out being Class I, the prognosis is always particularly good no matter if an extraction or non-extraction treatment plan is executed. (Fig. 1) Clinical confirmation needs to be made of the molar relationships bilaterally to determine if the molars are Class I, Class II, or Class III. (Fig. 2) If a case starts with Class II in the cuspids but the molars present with a Class I relationship, leveling the curve-of-Spee will be the primary treatment objective and required to finish with the cuspids Class I. (Fig. 3) Typically in these cases, eventual banding/bonding the lower 7’s in finishing to assist optimally leveling the lower curve-of-Spee. It is critically important to observe if the molars are Class I on one side but Class II (or Class III) on the other side, the cause of this must be determined to generate the correct treatment plan. Causes of the molars being Class I on one side yet Class II (or Class III) on the other side include: ᕡ Upper arch asymmetry ᕢ Lower arch asymmetry ᕣ A functional shift of the mandible ᕤ A combination of the above The Mythology of Mesial Drift In general, only upper molars tend to drift mesially if they have an opportunity to do so. The crowns of lower molars tend to tip mesially with minimal mesial movement of the roots. All of the other upper and lower 5-5 teeth tend to drift distally. In fact, if a correct generalization about how teeth drift, it would be distal drift and not mesial drift when teeth have an opportu-nity to do so. This is completely documentable when ceph overlays are taken over time after tooth loss. But it is as easy as looking at casts of patients that have lost teeth. Patients that lose upper first molars before age 30 without treatment seldom have Class II on the side of the missing upper 6’s. Distal drifting of the bicuspids and cuspids result in serendipitous Class II correction. On the other hand, if a patient loses a lower 6 rela-tively early in life, the distal drift of the lower bicuspids, cuspid, and incisors on the effected side result in the creation of Class II if the patient started out being Class I. Early loss of a lower 6 also often results in the correction of Class III if this was the starting occlusal condition. Cephs Can Indicate Upper Arch Asymmetry But there can be other important diagnostic informa-tion derived from looking at the first molar relationship. If there is no head positioning error, there should only be one upper first molar visible if the upper arch is symmetrical, as the left and right first molars should superimpose. But, if two distinct upper first molars are seen, this could be evidence of upper arch asymmetry that would influence Class II or Class III diagnosis and treatment planning. Confirmation of this can be made with an upper occlusal model or upper occlusal photo where perpendicular lines of the mesial molars relative to the mid-palatal suture are clearly not coincidental. Clini-cal facial inspection may also be helpful. (Figs. 4 & 5) Cephs Can Indicate Lower Arch Asymmetry Lower arches are rarely asymmetric unless there is premature loss of the lower E’s, lower 5’s, or lower 6’s. Basic empirical observation dispels any notion of “mesial drift.” Fig. 6 shows a missing lower right 5 case. Noteworthy is the quality of the bony ridge as a future implant site when opened orthodontically. And often when a patient is missing a lower 5 or lower 6, the treatment decision might best be to open up a lower 4 space to reduce treatment time or to create an implant site bearing less occlusal load. This would www.orthodontics.com Spring 2020 35
Journal of the American Orthodontic Society Spring 2020: Page 35