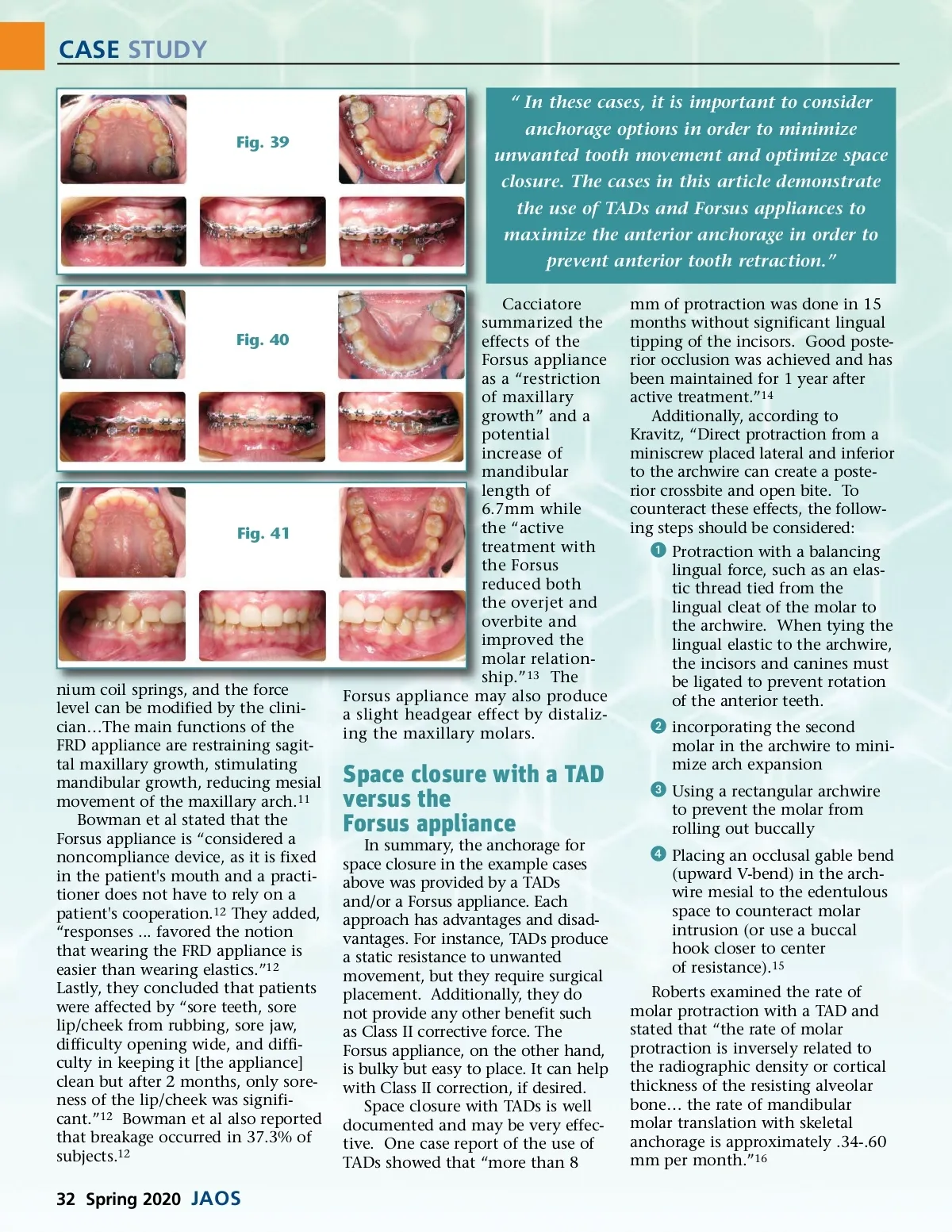
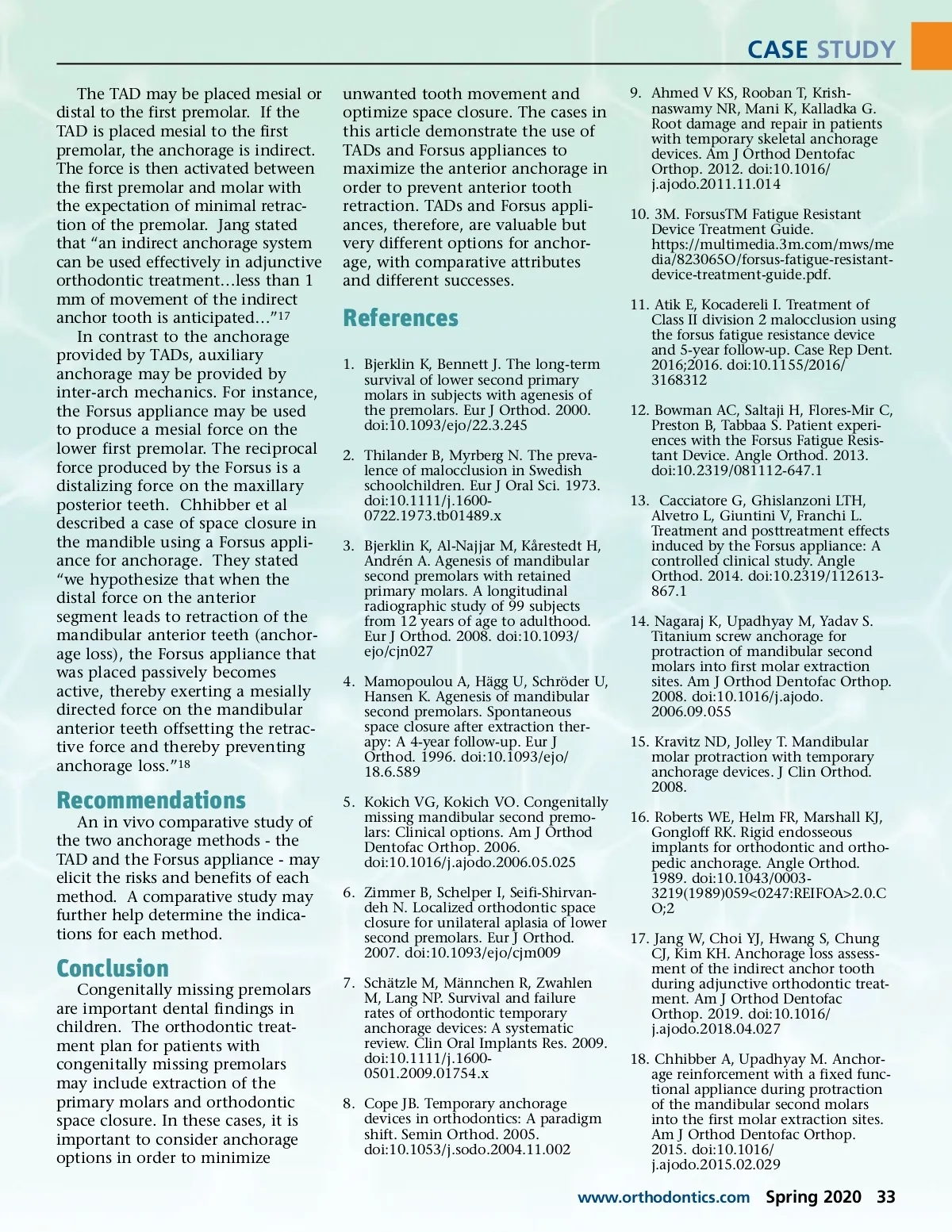
CASE STUDY “ In these cases, it is important to consider Fig. 39 anchorage options in order to minimize unwanted tooth movement and optimize space closure. The cases in this article demonstrate the use of TADs and Forsus appliances to maximize the anterior anchorage in order to prevent anterior tooth retraction.” Cacciatore summarized the effects of the Forsus appliance as a “restriction of maxillary growth” and a potential increase of mandibular length of 6.7mm while the “active treatment with the Forsus reduced both the overjet and overbite and improved the molar relation-ship.” 13 The Forsus appliance may also produce a slight headgear effect by distaliz-ing the maxillary molars. mm of protraction was done in 15 months without significant lingual tipping of the incisors. Good poste-rior occlusion was achieved and has been maintained for 1 year after active treatment.” 14 Additionally, according to Kravitz, “Direct protraction from a miniscrew placed lateral and inferior to the archwire can create a poste-rior crossbite and open bite. To counteract these effects, the follow-ing steps should be considered: ᕡ Protraction with a balancing lingual force, such as an elas-tic thread tied from the lingual cleat of the molar to the archwire. When tying the lingual elastic to the archwire, the incisors and canines must be ligated to prevent rotation of the anterior teeth. ᕢ incorporating the second molar in the archwire to mini-mize arch expansion ᕣ Using a rectangular archwire to prevent the molar from rolling out buccally ᕤ Placing an occlusal gable bend (upward V-bend) in the arch-wire mesial to the edentulous space to counteract molar intrusion (or use a buccal hook closer to center of resistance). 15 Roberts examined the rate of molar protraction with a TAD and stated that “the rate of molar protraction is inversely related to the radiographic density or cortical thickness of the resisting alveolar bone… the rate of mandibular molar translation with skeletal anchorage is approximately .34-.60 mm per month.” 16 Fig. 40 Fig. 41 nium coil springs, and the force level can be modified by the clini-cian…The main functions of the FRD appliance are restraining sagit-tal maxillary growth, stimulating mandibular growth, reducing mesial movement of the maxillary arch. 11 Bowman et al stated that the Forsus appliance is “considered a noncompliance device, as it is fixed in the patient's mouth and a practi-tioner does not have to rely on a patient's cooperation. 12 They added, “responses ... favored the notion that wearing the FRD appliance is easier than wearing elastics.” 12 Lastly, they concluded that patients were affected by “sore teeth, sore lip/cheek from rubbing, sore jaw, difficulty opening wide, and diffi-culty in keeping it [the appliance] clean but after 2 months, only sore-ness of the lip/cheek was signifi-cant.” 12 Bowman et al also reported that breakage occurred in 37.3% of subjects. 12 Space closure with a TAD versus the Forsus appliance In summary, the anchorage for space closure in the example cases above was provided by a TADs and/or a Forsus appliance. Each approach has advantages and disad-vantages. For instance, TADs produce a static resistance to unwanted movement, but they require surgical placement. Additionally, they do not provide any other benefit such as Class II corrective force. The Forsus appliance, on the other hand, is bulky but easy to place. It can help with Class II correction, if desired. Space closure with TADs is well documented and may be very effec-tive. One case report of the use of TADs showed that “more than 8 32 Spring 2020 JAOS
Journal of the American Orthodontic Society Spring 2020: Page 32