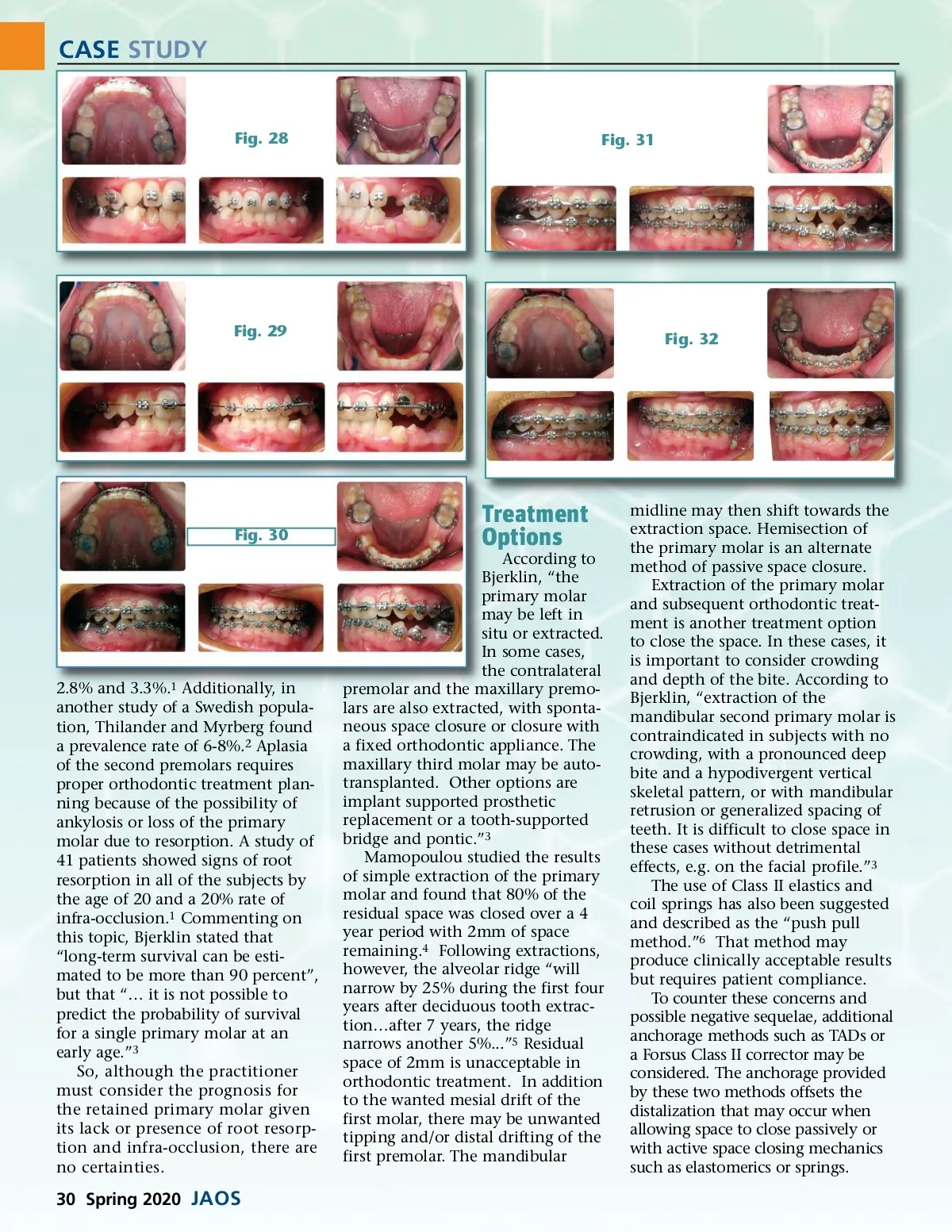
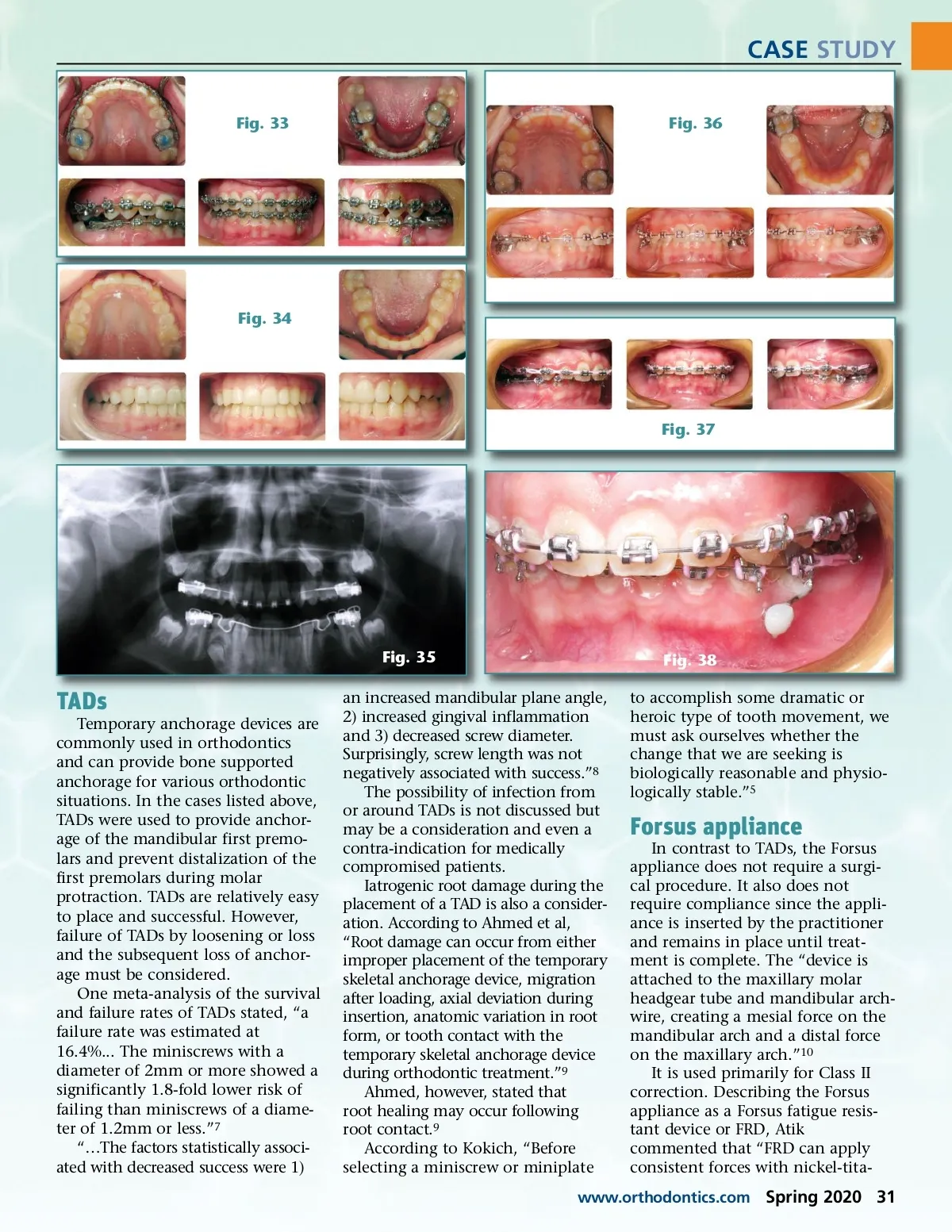
CASE STUDY Fig. 33 Fig. 36 Fig. 34 Fig. 37 Fig. 35 Fig. 38 to accomplish some dramatic or heroic type of tooth movement, we must ask ourselves whether the change that we are seeking is biologically reasonable and physio-logically stable.” 5 TADs Temporary anchorage devices are commonly used in orthodontics and can provide bone supported anchorage for various orthodontic situations. In the cases listed above, TADs were used to provide anchor-age of the mandibular first premo-lars and prevent distalization of the first premolars during molar protraction. TADs are relatively easy to place and successful. However, failure of TADs by loosening or loss and the subsequent loss of anchor-age must be considered. One meta-analysis of the survival and failure rates of TADs stated, “a failure rate was estimated at 16.4%... The miniscrews with a diameter of 2mm or more showed a significantly 1.8-fold lower risk of failing than miniscrews of a diame-ter of 1.2mm or less.” 7 “…The factors statistically associ-ated with decreased success were 1) an increased mandibular plane angle, 2) increased gingival inflammation and 3) decreased screw diameter. Surprisingly, screw length was not negatively associated with success.” 8 The possibility of infection from or around TADs is not discussed but may be a consideration and even a contra-indication for medically compromised patients. Iatrogenic root damage during the placement of a TAD is also a consider-ation. According to Ahmed et al, “Root damage can occur from either improper placement of the temporary skeletal anchorage device, migration after loading, axial deviation during insertion, anatomic variation in root form, or tooth contact with the temporary skeletal anchorage device during orthodontic treatment.” 9 Ahmed, however, stated that root healing may occur following root contact. 9 According to Kokich, “Before selecting a miniscrew or miniplate Forsus appliance In contrast to TADs, the Forsus appliance does not require a surgi-cal procedure. It also does not require compliance since the appli-ance is inserted by the practitioner and remains in place until treat-ment is complete. The “device is attached to the maxillary molar headgear tube and mandibular arch-wire, creating a mesial force on the mandibular arch and a distal force on the maxillary arch.” 10 It is used primarily for Class II correction. Describing the Forsus appliance as a Forsus fatigue resis-tant device or FRD, Atik commented that “FRD can apply consistent forces with nickel-tita-www.orthodontics.com Spring 2020 31
Journal of the American Orthodontic Society Spring 2020: Page 31