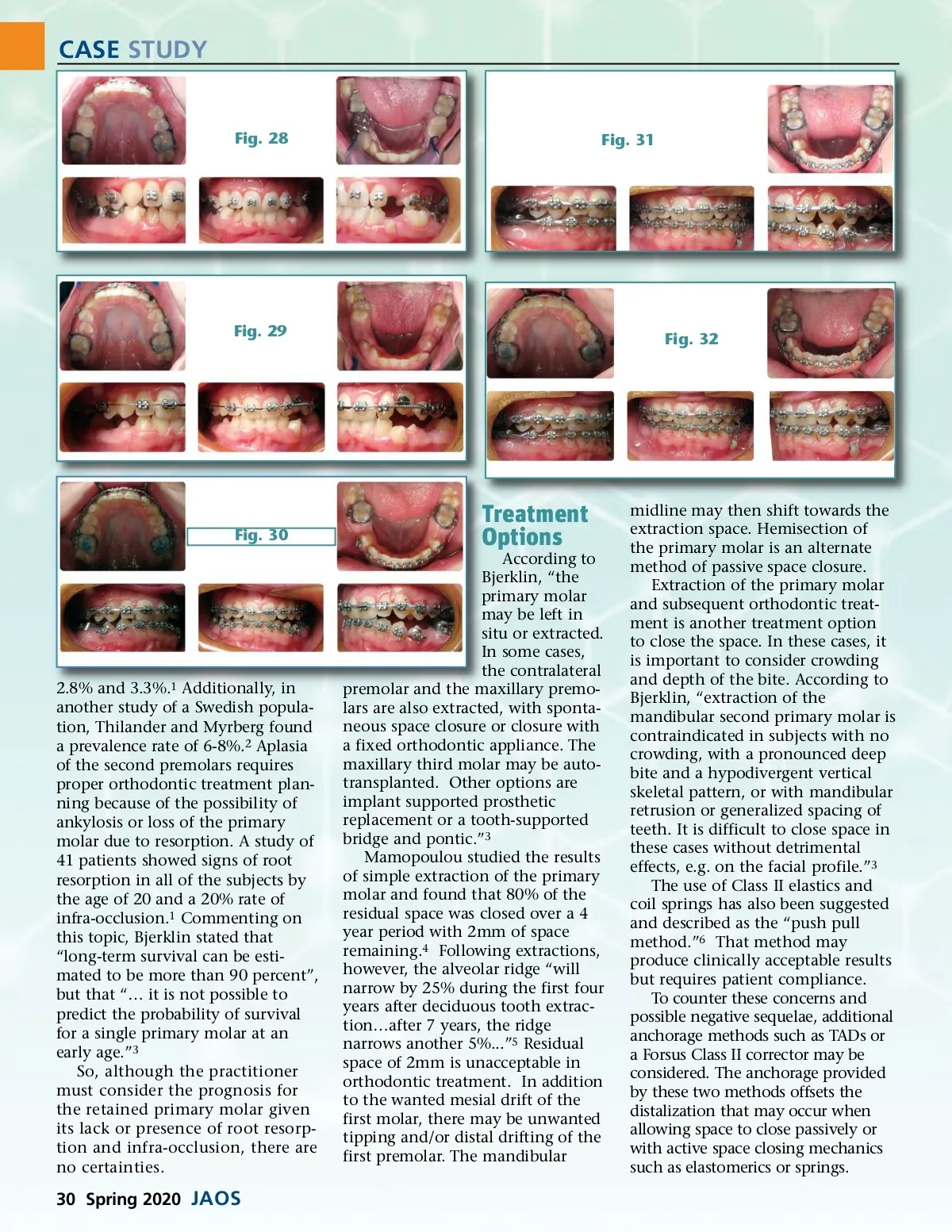
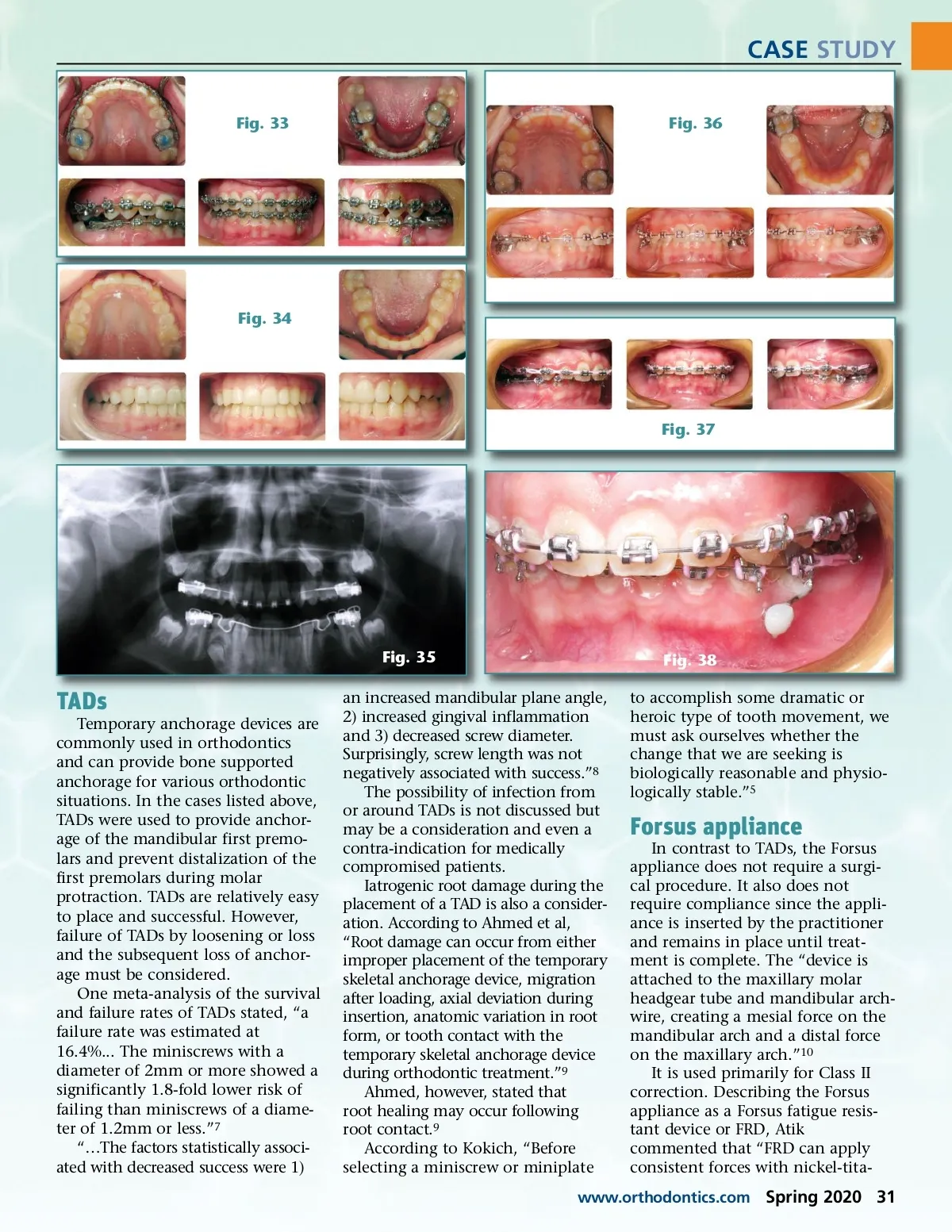
CASE STUDY Fig. 28 Fig. 31 Fig. 29 Fig. 32 Fig. 30 Treatment Options According to Bjerklin, “the primary molar may be left in situ or extracted. In some cases, the contralateral premolar and the maxillary premo-lars are also extracted, with sponta-neous space closure or closure with a fixed orthodontic appliance. The maxillary third molar may be auto-transplanted. Other options are implant supported prosthetic replacement or a tooth-supported bridge and pontic.” 3 Mamopoulou studied the results of simple extraction of the primary molar and found that 80% of the residual space was closed over a 4 year period with 2mm of space remaining. 4 Following extractions, however, the alveolar ridge “will narrow by 25% during the first four years after deciduous tooth extrac-tion…after 7 years, the ridge narrows another 5%...” 5 Residual space of 2mm is unacceptable in orthodontic treatment. In addition to the wanted mesial drift of the first molar, there may be unwanted tipping and/or distal drifting of the first premolar. The mandibular 2.8% and 3.3%. 1 Additionally, in another study of a Swedish popula-tion, Thilander and Myrberg found a prevalence rate of 6-8%. 2 Aplasia of the second premolars requires proper orthodontic treatment plan-ning because of the possibility of ankylosis or loss of the primary molar due to resorption. A study of 41 patients showed signs of root resorption in all of the subjects by the age of 20 and a 20% rate of infra-occlusion. 1 Commenting on this topic, Bjerklin stated that “long-term survival can be esti-mated to be more than 90 percent”, but that “… it is not possible to predict the probability of survival for a single primary molar at an early age.” 3 So, although the practitioner must consider the prognosis for the retained primary molar given its lack or presence of root resorp-tion and infra-occlusion, there are no certainties. midline may then shift towards the extraction space. Hemisection of the primary molar is an alternate method of passive space closure. Extraction of the primary molar and subsequent orthodontic treat-ment is another treatment option to close the space. In these cases, it is important to consider crowding and depth of the bite. According to Bjerklin, “extraction of the mandibular second primary molar is contraindicated in subjects with no crowding, with a pronounced deep bite and a hypodivergent vertical skeletal pattern, or with mandibular retrusion or generalized spacing of teeth. It is difficult to close space in these cases without detrimental effects, e.g. on the facial profile.” 3 The use of Class II elastics and coil springs has also been suggested and described as the “push pull method.” 6 That method may produce clinically acceptable results but requires patient compliance. To counter these concerns and possible negative sequelae, additional anchorage methods such as TADs or a Forsus Class II corrector may be considered. The anchorage provided by these two methods offsets the distalization that may occur when allowing space to close passively or with active space closing mechanics such as elastomerics or springs. 30 Spring 2020 JAOS
Journal of the American Orthodontic Society Spring 2020: Page 30