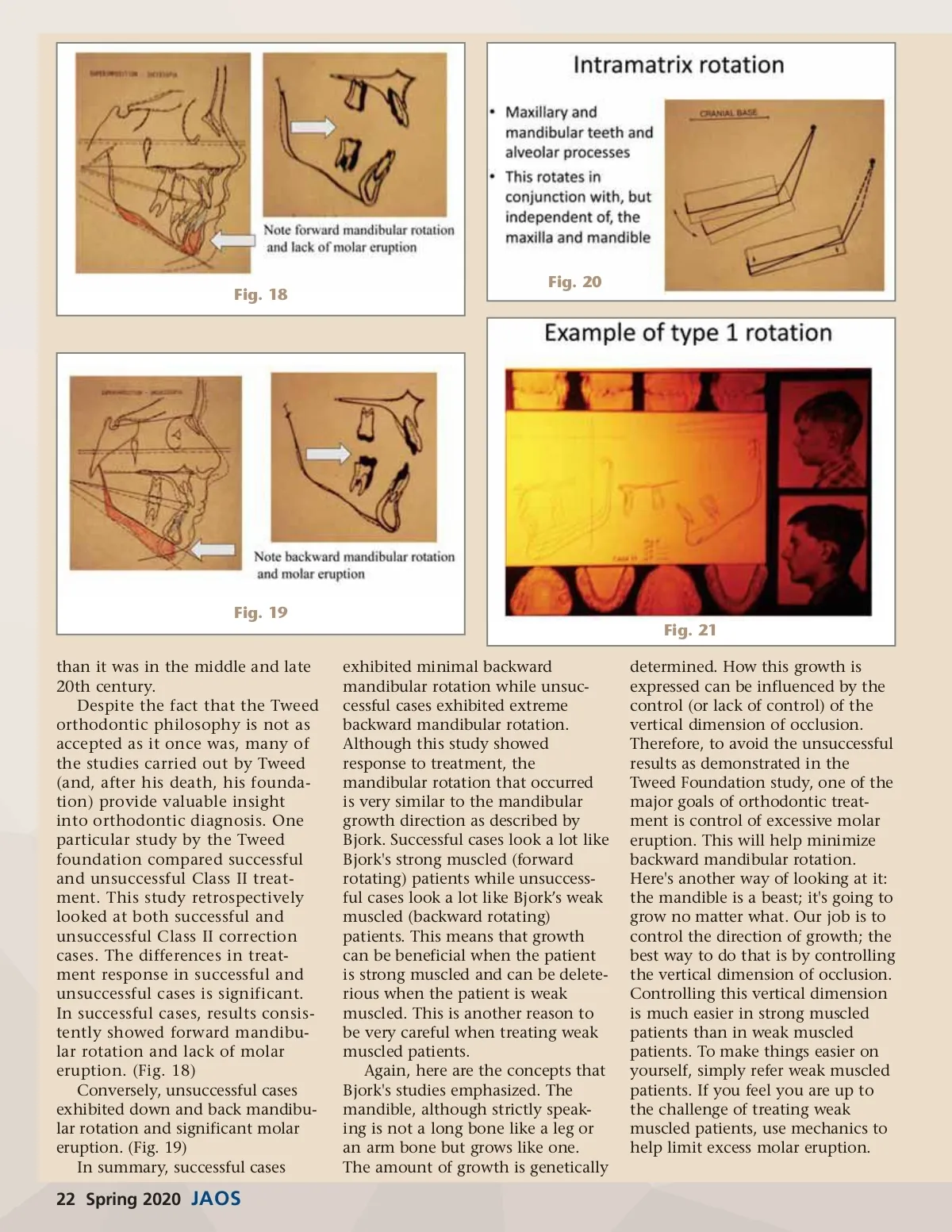
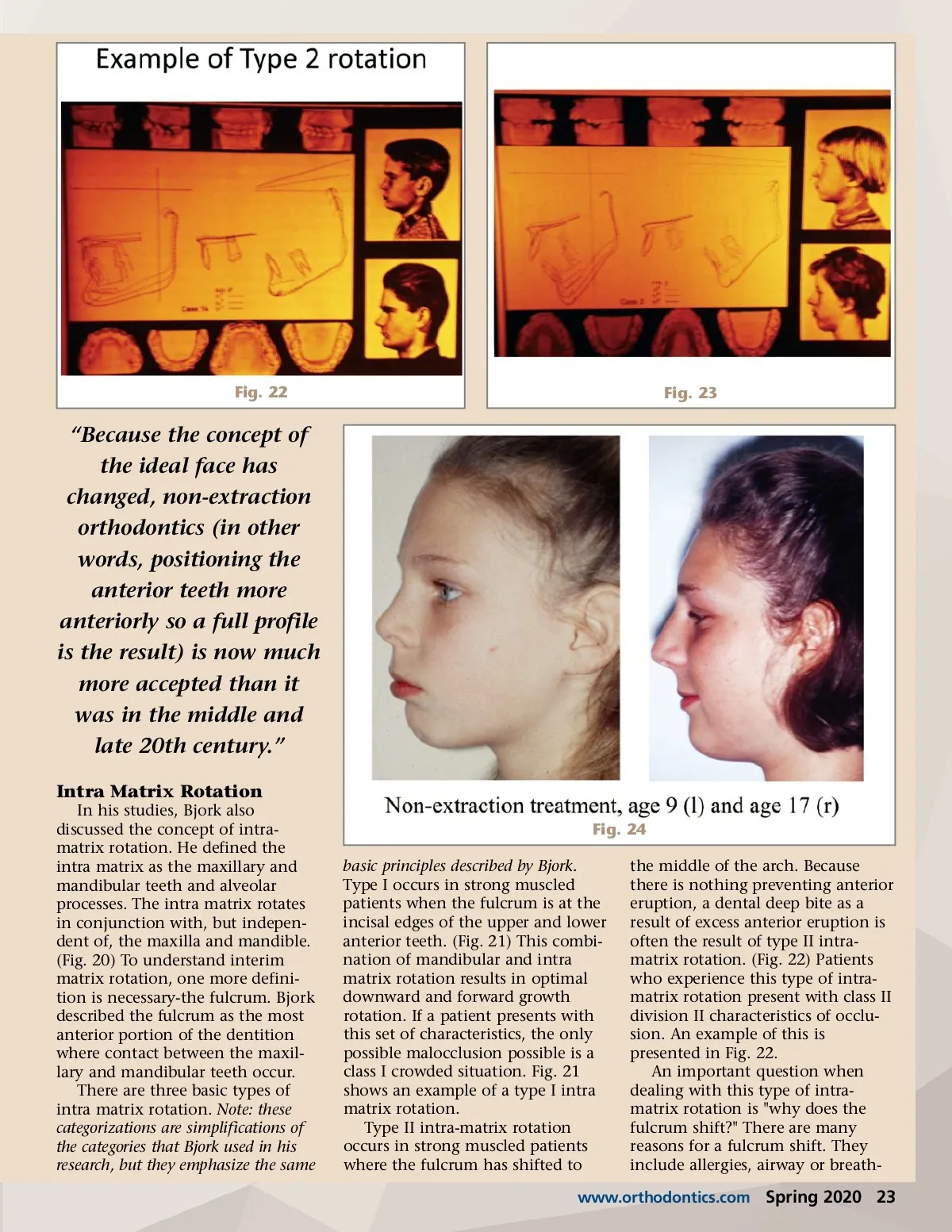
Fig. 18 Fig. 20 Fig. 19 Fig. 21 than it was in the middle and late 20th century. Despite the fact that the Tweed orthodontic philosophy is not as accepted as it once was, many of the studies carried out by Tweed (and, after his death, his founda-tion) provide valuable insight into orthodontic diagnosis. One particular study by the Tweed foundation compared successful and unsuccessful Class II treat-ment. This study retrospectively looked at both successful and unsuccessful Class II correction cases. The differences in treat-ment response in successful and unsuccessful cases is significant. In successful cases, results consis-tently showed forward mandibu-lar rotation and lack of molar eruption. (Fig. 18) Conversely, unsuccessful cases exhibited down and back mandibu-lar rotation and significant molar eruption. (Fig. 19) In summary, successful cases exhibited minimal backward mandibular rotation while unsuc-cessful cases exhibited extreme backward mandibular rotation. Although this study showed response to treatment, the mandibular rotation that occurred is very similar to the mandibular growth direction as described by Bjork. Successful cases look a lot like Bjork's strong muscled (forward rotating) patients while unsuccess-ful cases look a lot like Bjork’s weak muscled (backward rotating) patients. This means that growth can be beneficial when the patient is strong muscled and can be delete-rious when the patient is weak muscled. This is another reason to be very careful when treating weak muscled patients. Again, here are the concepts that Bjork's studies emphasized. The mandible, although strictly speak-ing is not a long bone like a leg or an arm bone but grows like one. The amount of growth is genetically determined. How this growth is expressed can be influenced by the control (or lack of control) of the vertical dimension of occlusion. Therefore, to avoid the unsuccessful results as demonstrated in the Tweed Foundation study, one of the major goals of orthodontic treat-ment is control of excessive molar eruption. This will help minimize backward mandibular rotation. Here's another way of looking at it: the mandible is a beast; it's going to grow no matter what. Our job is to control the direction of growth; the best way to do that is by controlling the vertical dimension of occlusion. Controlling this vertical dimension is much easier in strong muscled patients than in weak muscled patients. To make things easier on yourself, simply refer weak muscled patients. If you feel you are up to the challenge of treating weak muscled patients, use mechanics to help limit excess molar eruption. 22 Spring 2020 JAOS
Journal of the American Orthodontic Society Spring 2020: Page 22