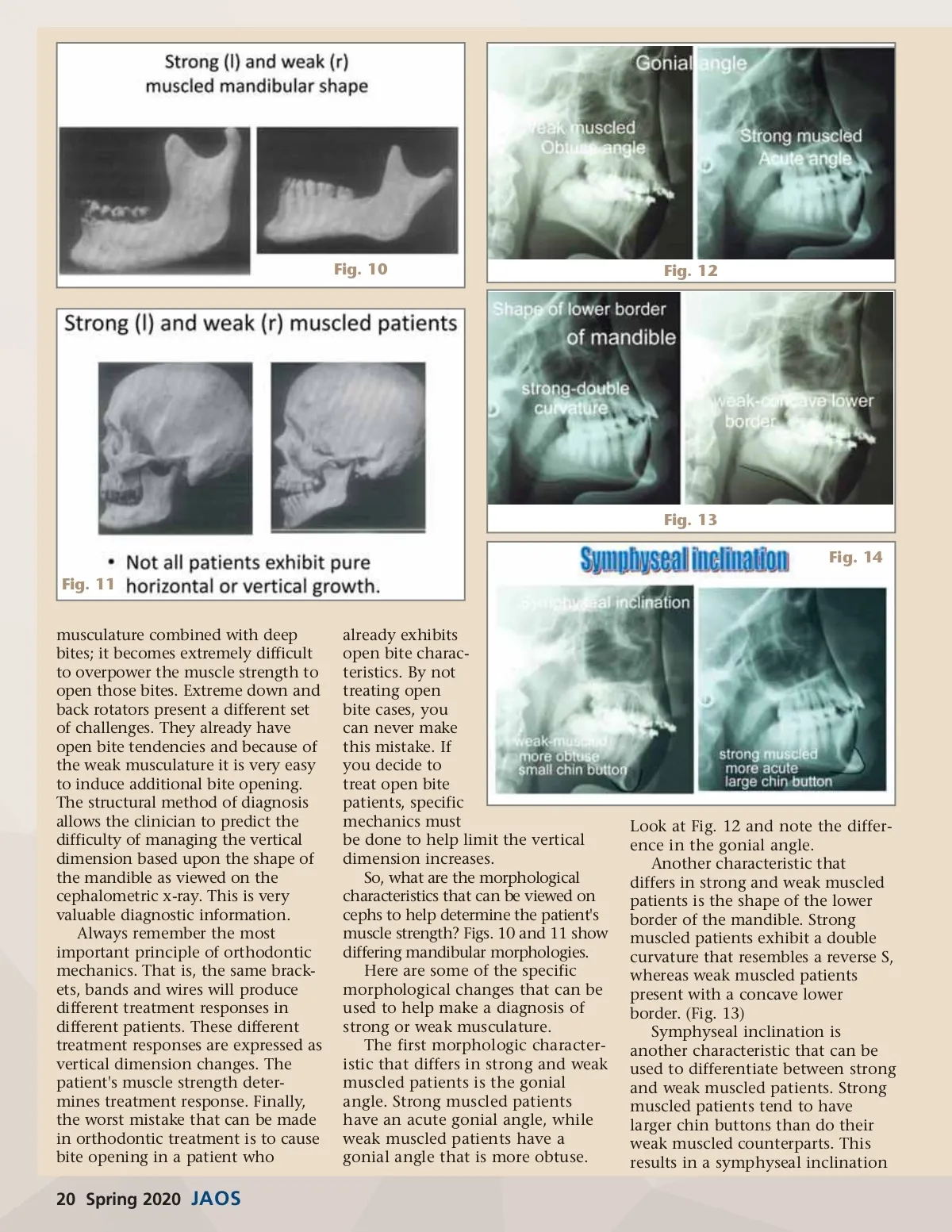
Fig. 15 Fig. 17 tion of growth rotation can be predicted. This knowledge (as you'll see later) is vitally important in orthodontic diagnosis. In summary, patients who exhibit extreme forward or extreme back-ward rotation have very distinct and different mandibular morphologies. Using mandibular morphology is an excellent diagnostic tool which enables the clinician to pick out the extreme forward and backward rota-tors. Patients who exhibit extremes in mandibular rotation are the most difficult cases to treat. In extreme forward rotators, the resulting deep bites are often difficult to correct because it is very difficult to over-power the strong muscles of mastica-tion. In extreme backroom rotators, exactly the opposite occurs. Open bites are very easily induced. There-fore the same orthodontic mechan-ics used in strong and weak muscled patients will produce vastly different results in the vertical dimension. This is the most important example of the number one rule in orthodon-tics-that is the same brackets, bands, and wires may and probably will produce different treatment responses in different patients. tics. Edward Angle is considered the father of modern orthodontics. He practiced around the turn-of-the-century and was an avowed non-extractionist. His rationale for treating all cases non-extraction was "God made the teeth, God made the bones, therefore they fit". Many of Angle’s students, particularly Dr. Charles Tweed, challenged Angle's insistence on non-extraction in all cases. This shows that the extraction/non-extraction debate is not new. Tweed felt that the best way to ensure long-term stability and facial balance in orthodontic cases was to position the mandibular incisors in an upright position. This required extractions in most cases. Because of Tweed's influ-ence, for most of the 20th century, extraction orthodontics dominated the scene. However, many studies have shown that the long-term stability of both extraction and non-extraction cases are approxi-mately the same. In other words, relapse is just as likely to occur in extraction and non-extraction cases. Furthermore, society's views on what constitutes a balanced face and pleasing profile has changed dramatically over the years. Fig. 17 illustrates how "ideal" facial balance has changed. Because the concept of the ideal face has changed, non-extraction orthodontics (in other words, posi-tioning the anterior teeth more anteriorly so a full profile is the result) is now much more accepted Fig. 16 that is acute in strong muscled patients, but more obtuse in weak muscled patients. (Fig. 14) Symphyseal radio-opacity or radio-lucency is another distin-guishing characteristic. Strong muscled patients tend to have thicker bone, and therefore a more radiopaque appearance, in the symphyseal area. Weak muscled patients are exactly the opposite-their symphyseal area tends to be more radiolucent. (Fig. 15) Finally, although it may be diffi-cult to see on a cephalometric x-ray, the inclination of the condyle differs in strong and weak muscled patients. Because the growth cells are located more in the anterior surface of the head of the condyle in strong muscled patients, condylar inclina-tion will be more in an anterior direction. Conversely, because the growth cells are located predomi-nantly on the posterior surface of the head of the condyle on weak muscled patients, condylar inclina-tion will be in a more posterior direc-tion. With the advent of 3D imaging, this characteristic is more observable compared to when viewed on a two-dimensional x-ray. (Fig. 16) By looking for these characteristics, muscle strength and therefore direc-An Orthodontic History Lesson To further understand some of the basics of orthodontic diagno-sis, it is important to understand some of the history of orthodon-www.orthodontics.com Spring 2020 21
Journal of the American Orthodontic Society Spring 2020: Page 21