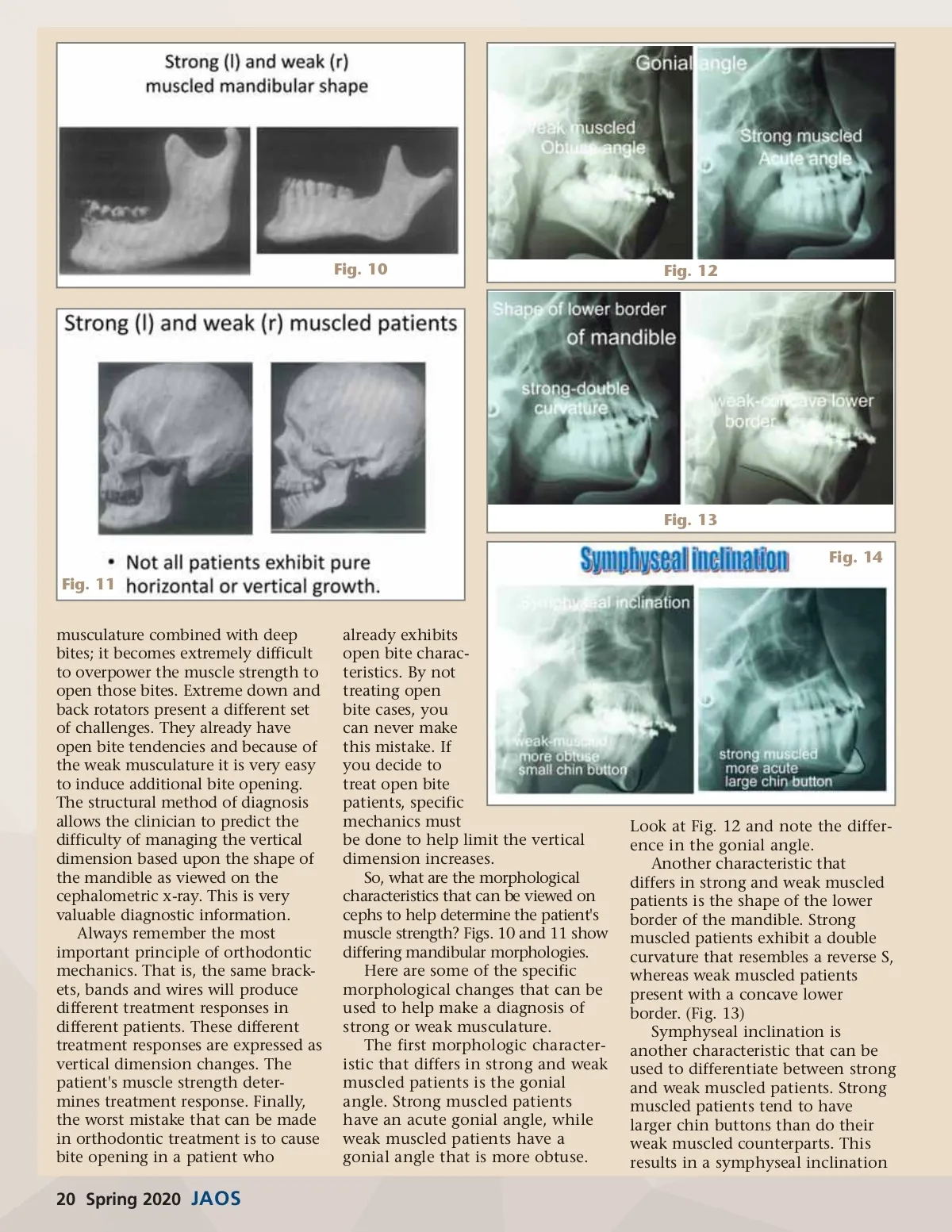
Fig. 10 Fig. 12 Fig. 13 Fig. 14 Fig. 11 musculature combined with deep bites; it becomes extremely difficult to overpower the muscle strength to open those bites. Extreme down and back rotators present a different set of challenges. They already have open bite tendencies and because of the weak musculature it is very easy to induce additional bite opening. The structural method of diagnosis allows the clinician to predict the difficulty of managing the vertical dimension based upon the shape of the mandible as viewed on the cephalometric x-ray. This is very valuable diagnostic information. Always remember the most important principle of orthodontic mechanics. That is, the same brack-ets, bands and wires will produce different treatment responses in different patients. These different treatment responses are expressed as vertical dimension changes. The patient's muscle strength deter-mines treatment response. Finally, the worst mistake that can be made in orthodontic treatment is to cause bite opening in a patient who already exhibits open bite charac-teristics. By not treating open bite cases, you can never make this mistake. If you decide to treat open bite patients, specific mechanics must be done to help limit the vertical dimension increases. So, what are the morphological characteristics that can be viewed on cephs to help determine the patient's muscle strength? Figs. 10 and 11 show differing mandibular morphologies. Here are some of the specific morphological changes that can be used to help make a diagnosis of strong or weak musculature. The first morphologic character-istic that differs in strong and weak muscled patients is the gonial angle. Strong muscled patients have an acute gonial angle, while weak muscled patients have a gonial angle that is more obtuse. Look at Fig. 12 and note the differ-ence in the gonial angle. Another characteristic that differs in strong and weak muscled patients is the shape of the lower border of the mandible. Strong muscled patients exhibit a double curvature that resembles a reverse S, whereas weak muscled patients present with a concave lower border. (Fig. 13) Symphyseal inclination is another characteristic that can be used to differentiate between strong and weak muscled patients. Strong muscled patients tend to have larger chin buttons than do their weak muscled counterparts. This results in a symphyseal inclination 20 Spring 2020 JAOS
Journal of the American Orthodontic Society Spring 2020: Page 20