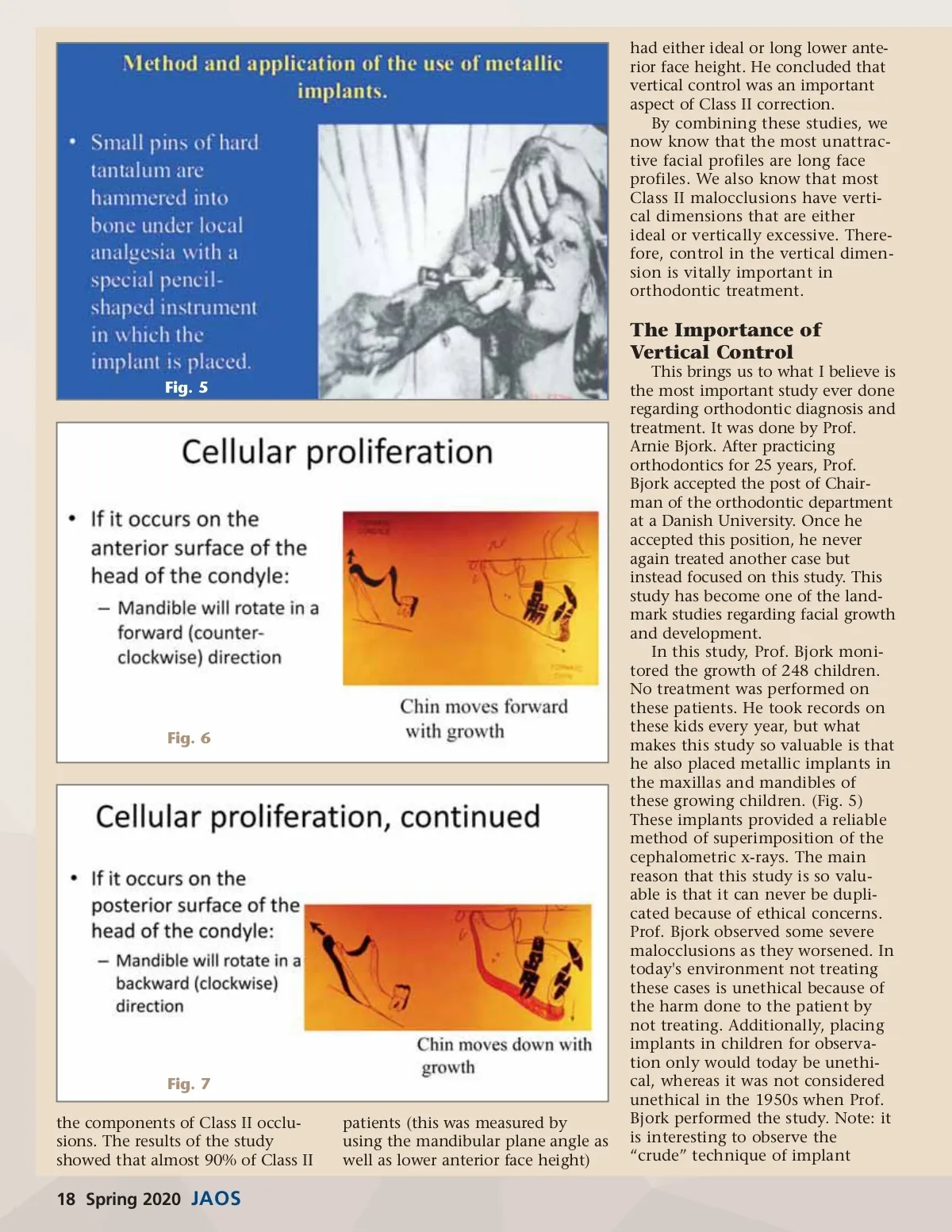
Fig. 8 placement. How will today’s “modern” techniques be viewed 50 years from now? What did Prof. Bjork conclude from this study? First, he postulated that the condyle is the driving force behind craniofacial development and that condylar growth direction depends upon the position of the growth cells which are located on the head of the condyle. This, he felt, is an inherited trait so the amount of mandibular growth is genetically determined. But, how this growth is expressed can be influenced by the control of the vertical dimension of occlusion. Prof. Bjork stated that if the growth cells are located on the anterior surface of the head of the condyle the mandible will rotate in a forward or counterclockwise direc-tion as growth occurs. (Fig. 6) Conversely if the growth cells are located on the posterior surface of the head of the condyle, the mandible will rotate in a downward or clockwise direction. (Fig. 7) Because of muscle size and the angle at which the muscles work differ in these two growth patterns, the forces of mastication are very different based upon growth rota-tion. In fact, the forces of occlusion can be up to six times more power-ful in forward rotating patients than in backward rotating patients. Because of this, forward rotating patients can be characterized as strong muscled patients and back-ward rotating patients can be char-acterized as weak muscled patients. Fig. 8 illustrates how the muscles work based on angles; it also shows that forward rotating patients have muscles that are stronger because they work more efficiently. Prof. Bjork also postulated that the location of growth cells can be anywhere on the condylar head, so most patients have some forward and some backward rotation charac-teristics. For our purposes, it is important to understand that the most difficult orthodontic cases are those patients that show extreme forward rotation (these would be very deep bite patients) and espe-cially extreme down and back rota-tion (these would be open bite patients). Because the muscles of mastication exert pressure and tension in different areas of the mandible depending on condylar growth direction, the shape or morphology of the mandible differs based upon growth direction. (Fig. 9) In other words, resorption and apposition of bone and therefore morphology of the mandible differs based upon growth direction. This provides the basis for what Bjork called the structural basis of deter-mining mandibular growth direc-tion. Therefore, growth direction can be predicted based upon mandibular morphology; this can be a very valuable diagnostic tool. As general dentist practicing orthodontics, it is good to know which cases are going to be the most difficult so we know what cases are candidates for referral. The structural method of determining growth direction enables the clini-cian to pick out the most difficult cases because the most extreme forward and downward rotators Fig. 9 have more distinctive mandibular morphological characteristics than do patients with more average growth rotation. So, this method identifies the extremes in growth rotation; this can be the basis for deciding whether the case should be referred. One of the most important aspects of orthodontic diagnosis is to recognize specific structural features that develop as a result of remodeling depending upon the direction of mandibular growth rotation. The rotation pattern can affect treatment. Most orthodontic mechanics are extrusive. Patients with a forward rotating growth pattern (these patients can be referred to as strong muscled patients) have masticatory muscles that can easily resist the extrusive component of most orthodontic mechanics. On the other hand, patients with a down and back rota-tional growth pattern (these patients can be referred to as a weak muscled patients) are often suscepti-ble to the extrusive component of orthodontic mechanics, because their muscles of mastication cannot overpower the extrusive component of the orthodontic mechanics. Since these weak muscled patients usually already have long faces, this extru-sion can be very harmful from an aesthetic and functional standpoint. Remember, Sassouni’s studies show that long faces are undesirable from an aesthetic standpoint. Extreme forward and extreme backward rotating patients are the most difficult cases to treat. Extreme forward rotators have very strong www.orthodontics.com Spring 2020 19
Journal of the American Orthodontic Society Spring 2020: Page 19