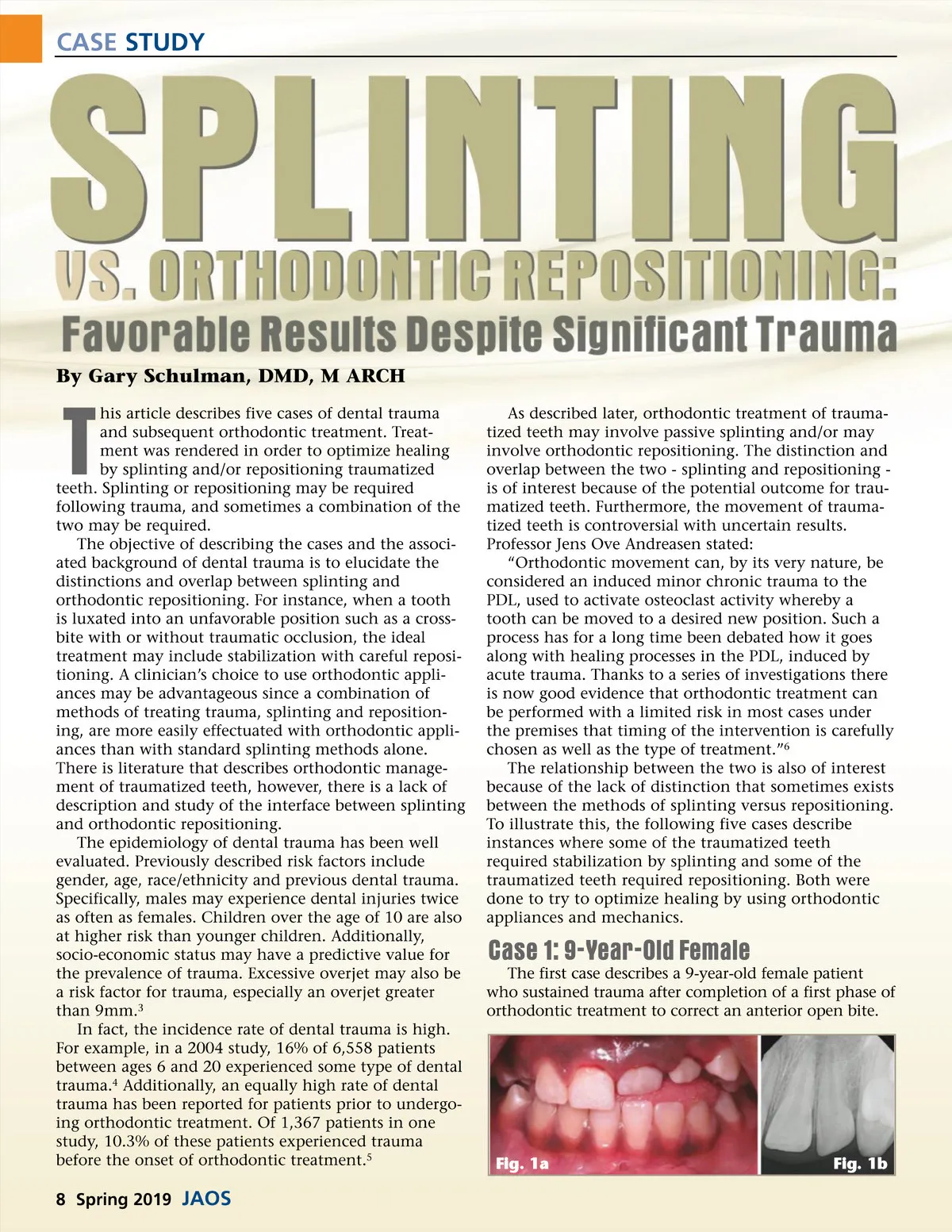
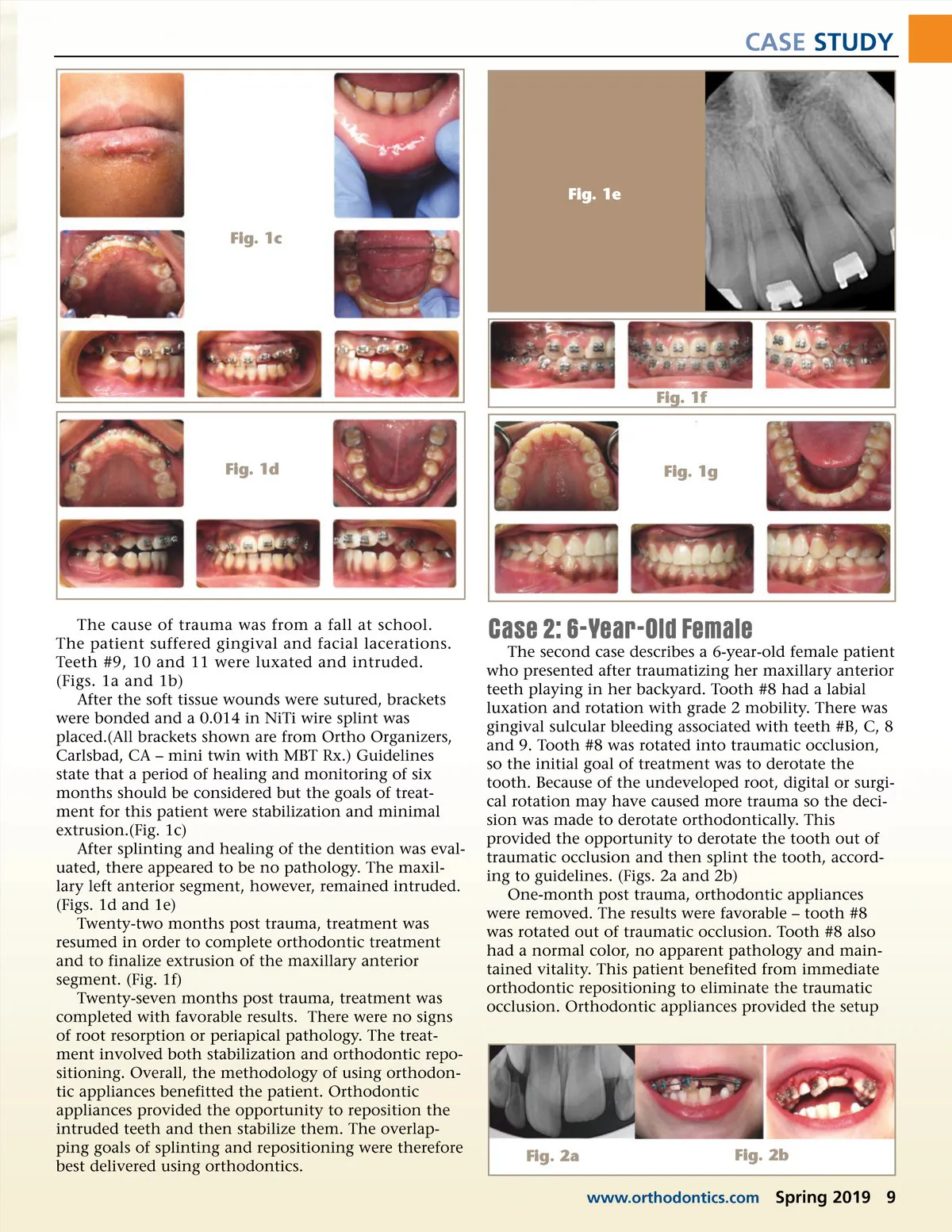
CASE STUDY Fig. 1e Fig. 1c Fig. 1f Fig. 1d Fig. 1g The cause of trauma was from a fall at school. The patient suffered gingival and facial lacerations. Teeth #9, 10 and 11 were luxated and intruded. (Figs. 1a and 1b) After the soft tissue wounds were sutured, brackets were bonded and a 0.014 in NiTi wire splint was placed.(All brackets shown are from Ortho Organizers, Carlsbad, CA – mini twin with MBT Rx.) Guidelines state that a period of healing and monitoring of six months should be considered but the goals of treat-ment for this patient were stabilization and minimal extrusion.(Fig. 1c) After splinting and healing of the dentition was eval-uated, there appeared to be no pathology. The maxil-lary left anterior segment, however, remained intruded. (Figs. 1d and 1e) Twenty-two months post trauma, treatment was resumed in order to complete orthodontic treatment and to finalize extrusion of the maxillary anterior segment. (Fig. 1f) Twenty-seven months post trauma, treatment was completed with favorable results. There were no signs of root resorption or periapical pathology. The treat-ment involved both stabilization and orthodontic repo-sitioning. Overall, the methodology of using orthodon-tic appliances benefitted the patient. Orthodontic appliances provided the opportunity to reposition the intruded teeth and then stabilize them. The overlap-ping goals of splinting and repositioning were therefore best delivered using orthodontics. Case 2: 6-Year-Old Female The second case describes a 6-year-old female patient who presented after traumatizing her maxillary anterior teeth playing in her backyard. Tooth #8 had a labial luxation and rotation with grade 2 mobility. There was gingival sulcular bleeding associated with teeth #B, C, 8 and 9. Tooth #8 was rotated into traumatic occlusion, so the initial goal of treatment was to derotate the tooth. Because of the undeveloped root, digital or surgi-cal rotation may have caused more trauma so the deci-sion was made to derotate orthodontically. This provided the opportunity to derotate the tooth out of traumatic occlusion and then splint the tooth, accord-ing to guidelines. (Figs. 2a and 2b) One-month post trauma, orthodontic appliances were removed. The results were favorable – tooth #8 was rotated out of traumatic occlusion. Tooth #8 also had a normal color, no apparent pathology and main-tained vitality. This patient benefited from immediate orthodontic repositioning to eliminate the traumatic occlusion. Orthodontic appliances provided the setup Fig. 2a Fig. 2b www.orthodontics.com Spring 2019 9
Journal of the American Orthodontic Society Spring 2019: Page 9