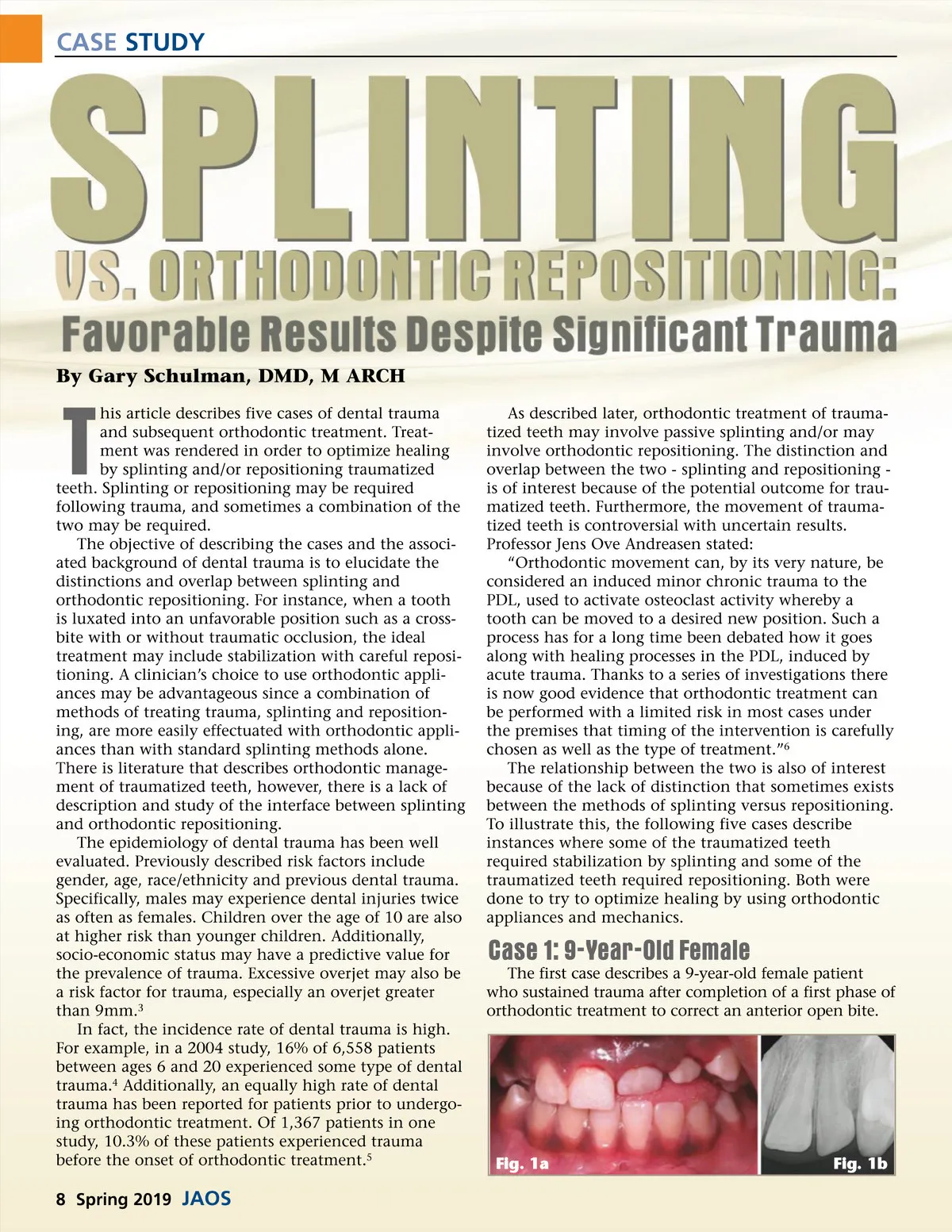
CASE STUDY By Gary Schulman, DMD, M ARCH his article describes five cases of dental trauma and subsequent orthodontic treatment. Treat-ment was rendered in order to optimize healing by splinting and/or repositioning traumatized teeth. Splinting or repositioning may be required following trauma, and sometimes a combination of the two may be required. The objective of describing the cases and the associ-ated background of dental trauma is to elucidate the distinctions and overlap between splinting and orthodontic repositioning. For instance, when a tooth is luxated into an unfavorable position such as a cross-bite with or without traumatic occlusion, the ideal treatment may include stabilization with careful reposi-tioning. A clinician’s choice to use orthodontic appli-ances may be advantageous since a combination of methods of treating trauma, splinting and reposition-ing, are more easily effectuated with orthodontic appli-ances than with standard splinting methods alone. There is literature that describes orthodontic manage-ment of traumatized teeth, however, there is a lack of description and study of the interface between splinting and orthodontic repositioning. The epidemiology of dental trauma has been well evaluated. Previously described risk factors include gender, age, race/ethnicity and previous dental trauma. Specifically, males may experience dental injuries twice as often as females. Children over the age of 10 are also at higher risk than younger children. Additionally, socio-economic status may have a predictive value for the prevalence of trauma. Excessive overjet may also be a risk factor for trauma, especially an overjet greater than 9mm. 3 In fact, the incidence rate of dental trauma is high. For example, in a 2004 study, 16% of 6,558 patients between ages 6 and 20 experienced some type of dental trauma. 4 Additionally, an equally high rate of dental trauma has been reported for patients prior to undergo-ing orthodontic treatment. Of 1,367 patients in one study, 10.3% of these patients experienced trauma before the onset of orthodontic treatment. 5 T As described later, orthodontic treatment of trauma-tized teeth may involve passive splinting and/or may involve orthodontic repositioning. The distinction and overlap between the two -splinting and repositioning -is of interest because of the potential outcome for trau-matized teeth. Furthermore, the movement of trauma-tized teeth is controversial with uncertain results. Professor Jens Ove Andreasen stated: “Orthodontic movement can, by its very nature, be considered an induced minor chronic trauma to the PDL, used to activate osteoclast activity whereby a tooth can be moved to a desired new position. Such a process has for a long time been debated how it goes along with healing processes in the PDL, induced by acute trauma. Thanks to a series of investigations there is now good evidence that orthodontic treatment can be performed with a limited risk in most cases under the premises that timing of the intervention is carefully chosen as well as the type of treatment.” 6 The relationship between the two is also of interest because of the lack of distinction that sometimes exists between the methods of splinting versus repositioning. To illustrate this, the following five cases describe instances where some of the traumatized teeth required stabilization by splinting and some of the traumatized teeth required repositioning. Both were done to try to optimize healing by using orthodontic appliances and mechanics. Case 1: 9-Year-Old Female The first case describes a 9-year-old female patient who sustained trauma after completion of a first phase of orthodontic treatment to correct an anterior open bite. Fig. 1a Fig. 1b 8 Spring 2019 JAOS
Journal of the American Orthodontic Society Spring 2019: Page 8