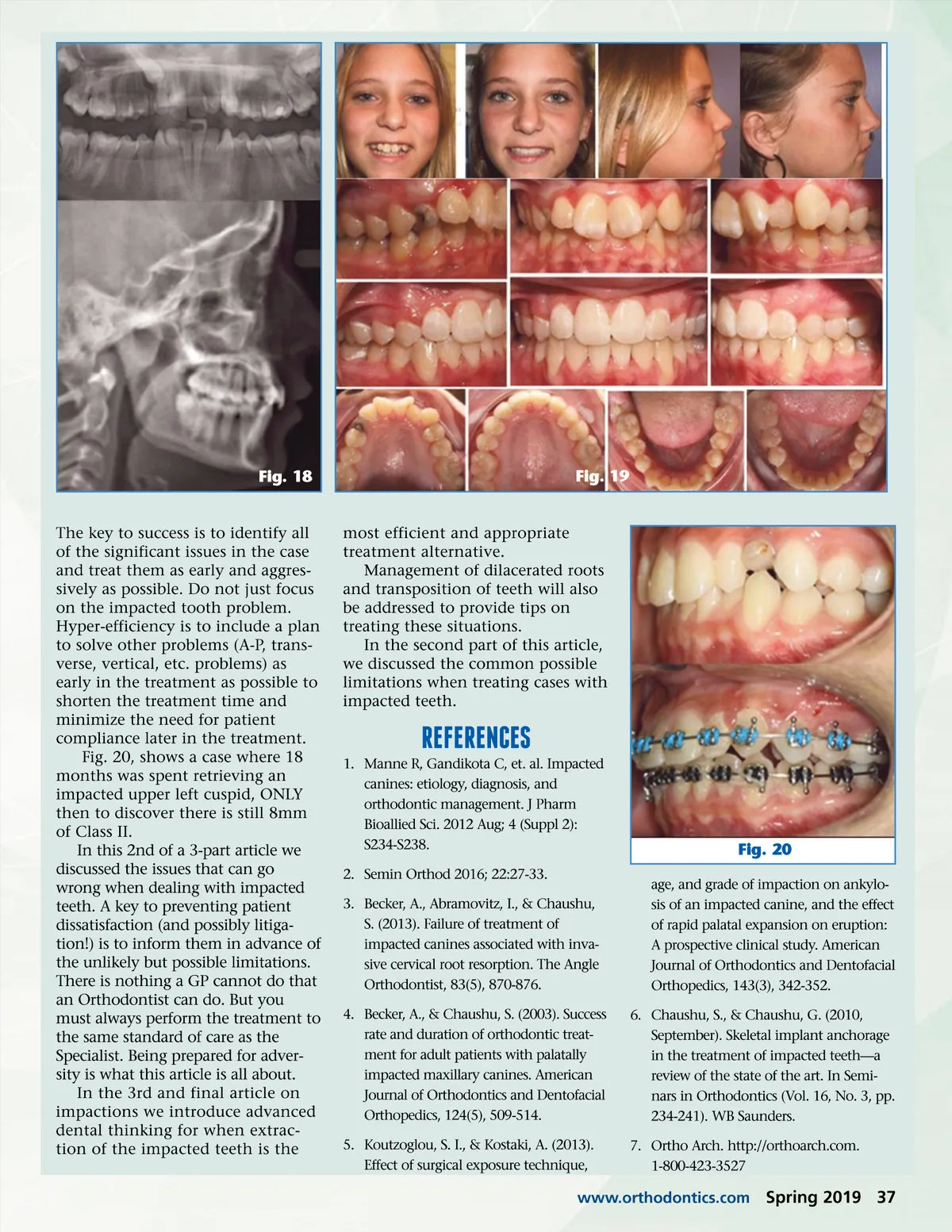
Fig. 15 Fig. 17 Fig. 16 they are the “cornerstone of the arch” has proven to be incorrect. Patients congenitally missing upper lateral incisors and have the cuspids substitute as laterals and the first bicuspids substitute as the cuspids have no functional or TMD issues. So it turns out it is less essential to have the actual cuspid in the cuspid position than it is to have a natural tooth (with a PDL) in the cuspid position. (Figs. 13-17) lutely must be retrieved and it is impacted entirely within the alveo-lus, perhaps it is best to allow an Orthodontic Specialist to experience the joy of treating these cases. Later, we will share some advanced dental thinking proposing treatment plans that involve extrac-tion of impacted cuspids to dramat-ically speed treatment times and improve outcomes. The Case May Ultimately Require Restorative Treatment and Additional Costs There are cases with impacted teeth that ultimately could benefit from some restorative or aesthetic treatment. In this case an upper right cuspid was retrieved only to discover it was rotated 180 degrees. It might have required an additional year just to fully de-rotate this cuspid and the decision was made to bond some composite to improve the aesthetic outcome. (Fig. 10-11) In another case an impacted cuspid was retrieved only to discover it had a cementoma and mucogingival defect that required additional extrusion and a restora-tion to get an acceptable aesthetic result. (Fig. 12) Note: Intentional extrusion of teeth is often best accom-plished using .021”x.025” Turbo Braid 8 to optimize bodily movement with-out tipping. There is a traditional troglodyte thinking of the dental profession that “cuspids are sacred,” this ignores the long term aesthetic and func-tional success of cases treated with extraction of cuspids. the defInItIon of advanced dental thInKIng: WorK smarter not harder One of the biggest mistakes made when treating a case with an impacted tooth is to get “tunnel visioned” on the impacted tooth issue. Many will work for 2 years (or more) to retrieve and align the impacted cuspid only to later discover there is also a full 8mm of Class II bilaterally. Consider the following example case with a full 8mm of Class II and an impacted upper right cuspid. Note how much faster and easier the case treated out with extraction of the upper cuspids. (Figs. 18-19) Or what about that posterior crossbite, arch asymmetry, profile considerations, or other issues that should be addressed in addition to the impacted tooth issue. It can be particularly difficult to get compli-ance from a patient that has already been in braces for 2 years or more. What If an upper Impacted tooth cannot be retrIeved? If an impacted cuspid cannot be retrieved the question arises how to restore the case. The authors believe implants do very well with vertical loading forces but not so well with the lateral excursive forces required by a canine. It may be best to mesialize the first bicuspid into the cuspid position and then place an implant in the upper first bicus-pid position. The notion that it is essential to retain the cuspids as 36 Spring 2019 JAOS
Journal of the American Orthodontic Society Spring 2019: Page 36