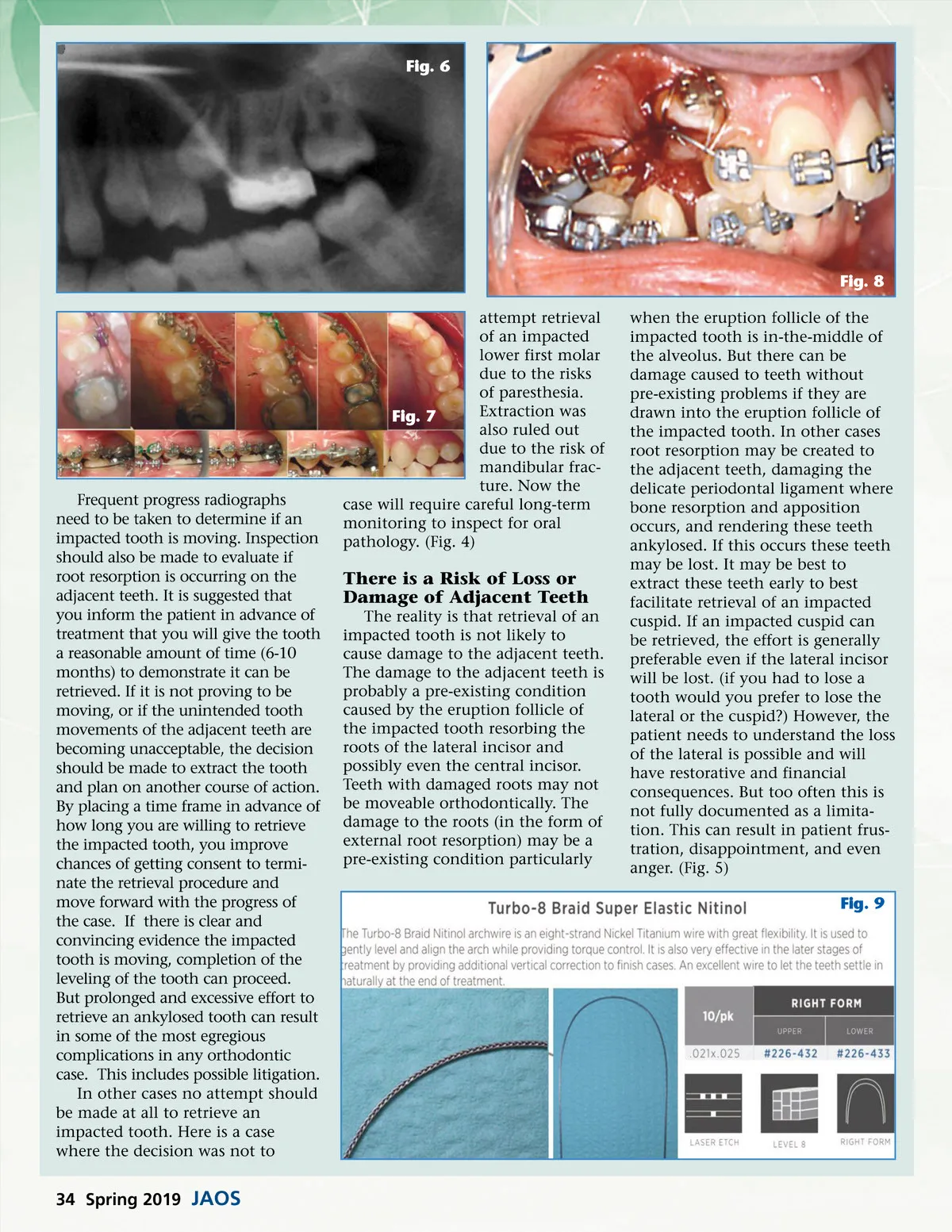
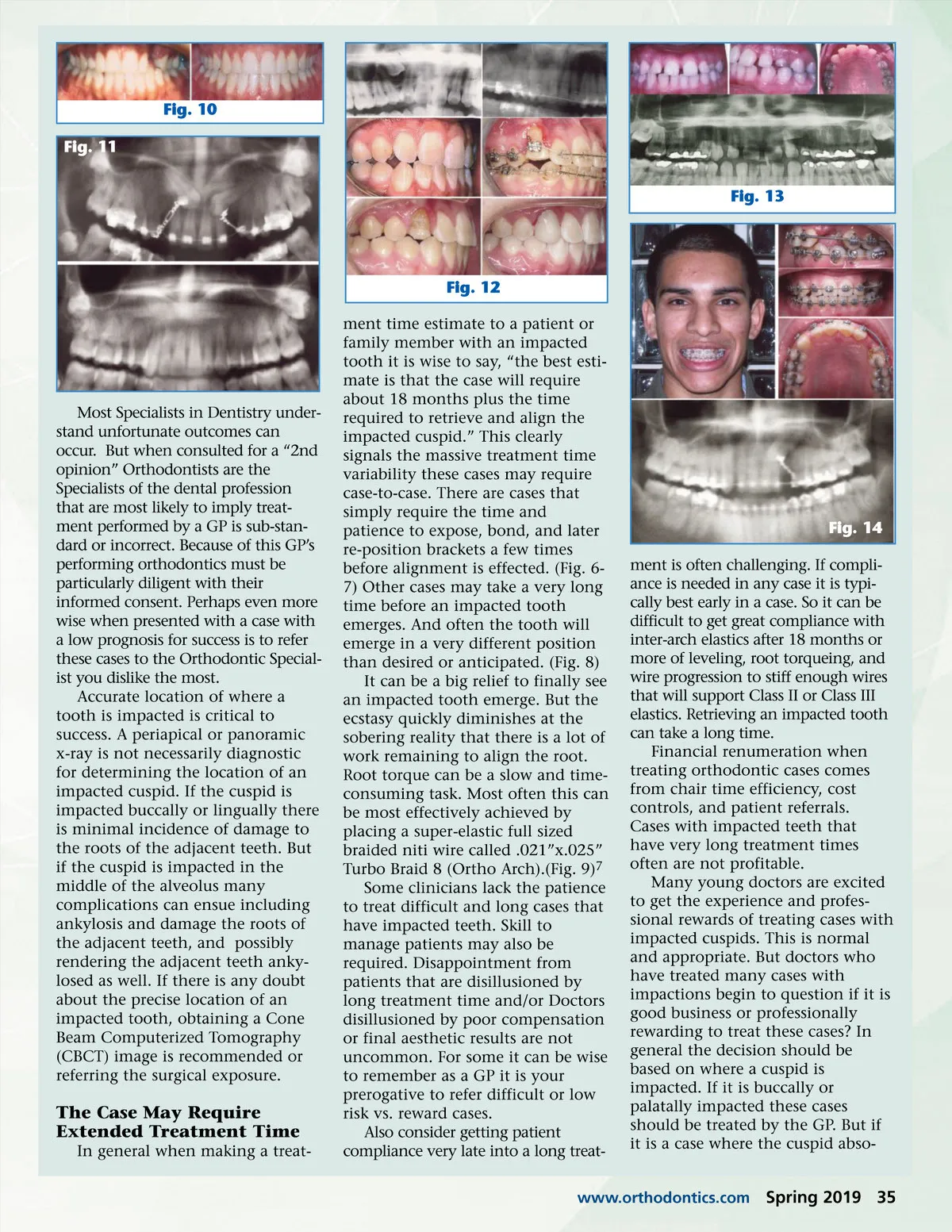
Fig. 10 Fig. 11 Fig. 13 Fig. 12 ment time estimate to a patient or family member with an impacted tooth it is wise to say, “the best esti-mate is that the case will require about 18 months plus the time required to retrieve and align the impacted cuspid.” This clearly signals the massive treatment time variability these cases may require case-to-case. There are cases that simply require the time and patience to expose, bond, and later re-position brackets a few times before alignment is effected. (Fig. 6-7) Other cases may take a very long time before an impacted tooth emerges. And often the tooth will emerge in a very different position than desired or anticipated. (Fig. 8) It can be a big relief to finally see an impacted tooth emerge. But the ecstasy quickly diminishes at the sobering reality that there is a lot of work remaining to align the root. Root torque can be a slow and time-consuming task. Most often this can be most effectively achieved by placing a super-elastic full sized braided niti wire called .021”x.025” Turbo Braid 8 (Ortho Arch).(Fig. 9) 7 Some clinicians lack the patience to treat difficult and long cases that have impacted teeth. Skill to manage patients may also be required. Disappointment from patients that are disillusioned by long treatment time and/or Doctors disillusioned by poor compensation or final aesthetic results are not uncommon. For some it can be wise to remember as a GP it is your prerogative to refer difficult or low risk vs. reward cases. Also consider getting patient compliance very late into a long treat-Most Specialists in Dentistry under-stand unfortunate outcomes can occur. But when consulted for a “2nd opinion” Orthodontists are the Specialists of the dental profession that are most likely to imply treat-ment performed by a GP is sub-stan-dard or incorrect. Because of this GP’s performing orthodontics must be particularly diligent with their informed consent. Perhaps even more wise when presented with a case with a low prognosis for success is to refer these cases to the Orthodontic Special-ist you dislike the most. Accurate location of where a tooth is impacted is critical to success. A periapical or panoramic x-ray is not necessarily diagnostic for determining the location of an impacted cuspid. If the cuspid is impacted buccally or lingually there is minimal incidence of damage to the roots of the adjacent teeth. But if the cuspid is impacted in the middle of the alveolus many complications can ensue including ankylosis and damage the roots of the adjacent teeth, and possibly rendering the adjacent teeth anky-losed as well. If there is any doubt about the precise location of an impacted tooth, obtaining a Cone Beam Computerized Tomography (CBCT) image is recommended or referring the surgical exposure. Fig. 14 ment is often challenging. If compli-ance is needed in any case it is typi-cally best early in a case. So it can be difficult to get great compliance with inter-arch elastics after 18 months or more of leveling, root torqueing, and wire progression to stiff enough wires that will support Class II or Class III elastics. Retrieving an impacted tooth can take a long time. Financial renumeration when treating orthodontic cases comes from chair time efficiency, cost controls, and patient referrals. Cases with impacted teeth that have very long treatment times often are not profitable. Many young doctors are excited to get the experience and profes-sional rewards of treating cases with impacted cuspids. This is normal and appropriate. But doctors who have treated many cases with impactions begin to question if it is good business or professionally rewarding to treat these cases? In general the decision should be based on where a cuspid is impacted. If it is buccally or palatally impacted these cases should be treated by the GP. But if it is a case where the cuspid abso-The Case May Require Extended Treatment Time In general when making a treat-www.orthodontics.com Spring 2019 35
Journal of the American Orthodontic Society Spring 2019: Page 35