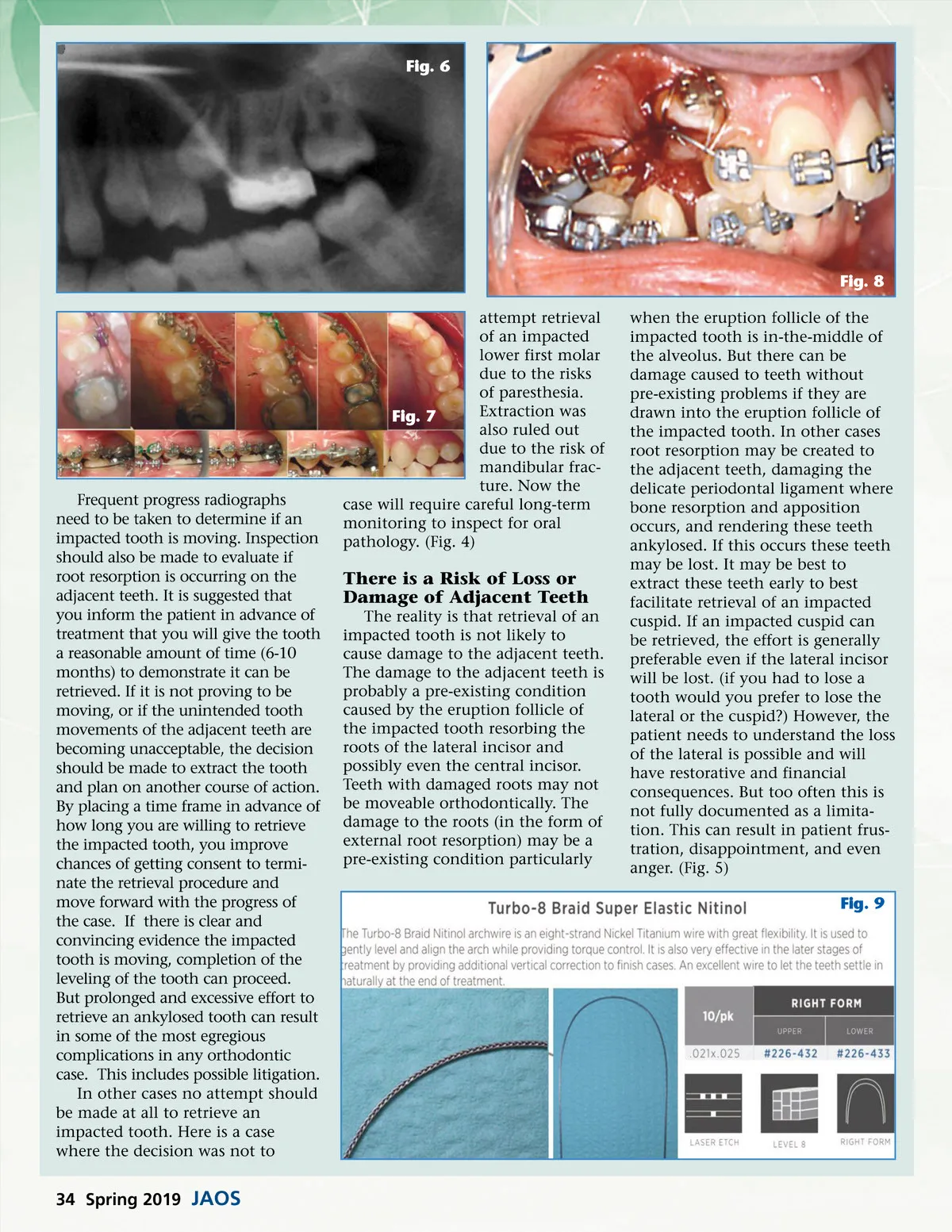
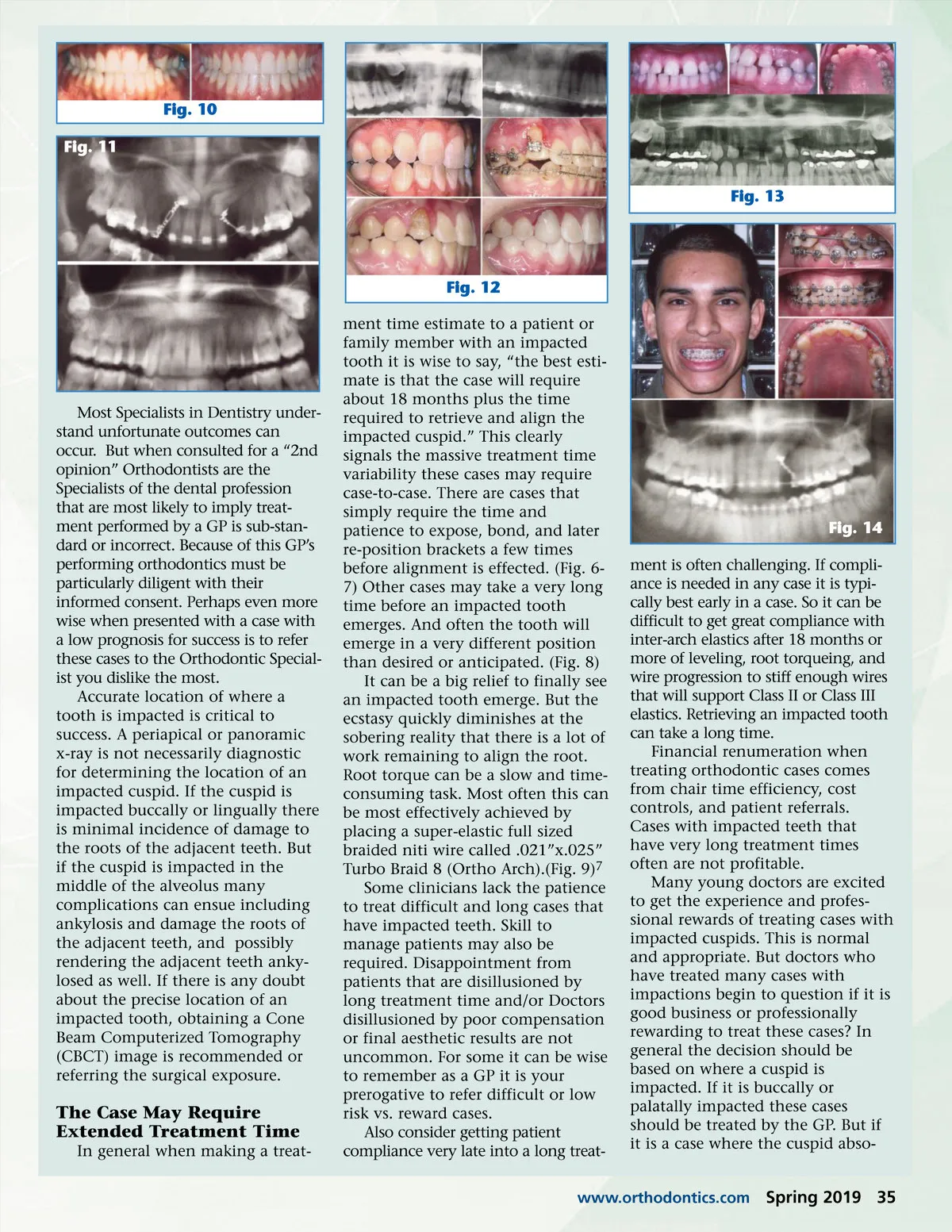
Fig. 6 Fig. 8 attempt retrieval of an impacted lower first molar due to the risks of paresthesia. Extraction was Fig. 7 also ruled out due to the risk of mandibular frac-ture. Now the case will require careful long-term monitoring to inspect for oral pathology. (Fig. 4) when the eruption follicle of the impacted tooth is in-the-middle of the alveolus. But there can be damage caused to teeth without pre-existing problems if they are drawn into the eruption follicle of the impacted tooth. In other cases root resorption may be created to the adjacent teeth, damaging the delicate periodontal ligament where bone resorption and apposition occurs, and rendering these teeth ankylosed. If this occurs these teeth may be lost. It may be best to extract these teeth early to best facilitate retrieval of an impacted cuspid. If an impacted cuspid can be retrieved, the effort is generally preferable even if the lateral incisor will be lost. (if you had to lose a tooth would you prefer to lose the lateral or the cuspid?) However, the patient needs to understand the loss of the lateral is possible and will have restorative and financial consequences. But too often this is not fully documented as a limita-tion. This can result in patient frus-tration, disappointment, and even anger. (Fig. 5) Fig. 9 Frequent progress radiographs need to be taken to determine if an impacted tooth is moving. Inspection should also be made to evaluate if root resorption is occurring on the adjacent teeth. It is suggested that you inform the patient in advance of treatment that you will give the tooth a reasonable amount of time (6-10 months) to demonstrate it can be retrieved. If it is not proving to be moving, or if the unintended tooth movements of the adjacent teeth are becoming unacceptable, the decision should be made to extract the tooth and plan on another course of action. By placing a time frame in advance of how long you are willing to retrieve the impacted tooth, you improve chances of getting consent to termi-nate the retrieval procedure and move forward with the progress of the case. If there is clear and convincing evidence the impacted tooth is moving, completion of the leveling of the tooth can proceed. But prolonged and excessive effort to retrieve an ankylosed tooth can result in some of the most egregious complications in any orthodontic case. This includes possible litigation. In other cases no attempt should be made at all to retrieve an impacted tooth. Here is a case where the decision was not to There is a Risk of Loss or Damage of Adjacent Teeth The reality is that retrieval of an impacted tooth is not likely to cause damage to the adjacent teeth. The damage to the adjacent teeth is probably a pre-existing condition caused by the eruption follicle of the impacted tooth resorbing the roots of the lateral incisor and possibly even the central incisor. Teeth with damaged roots may not be moveable orthodontically. The damage to the roots (in the form of external root resorption) may be a pre-existing condition particularly 34 Spring 2019 JAOS
Journal of the American Orthodontic Society Spring 2019: Page 34