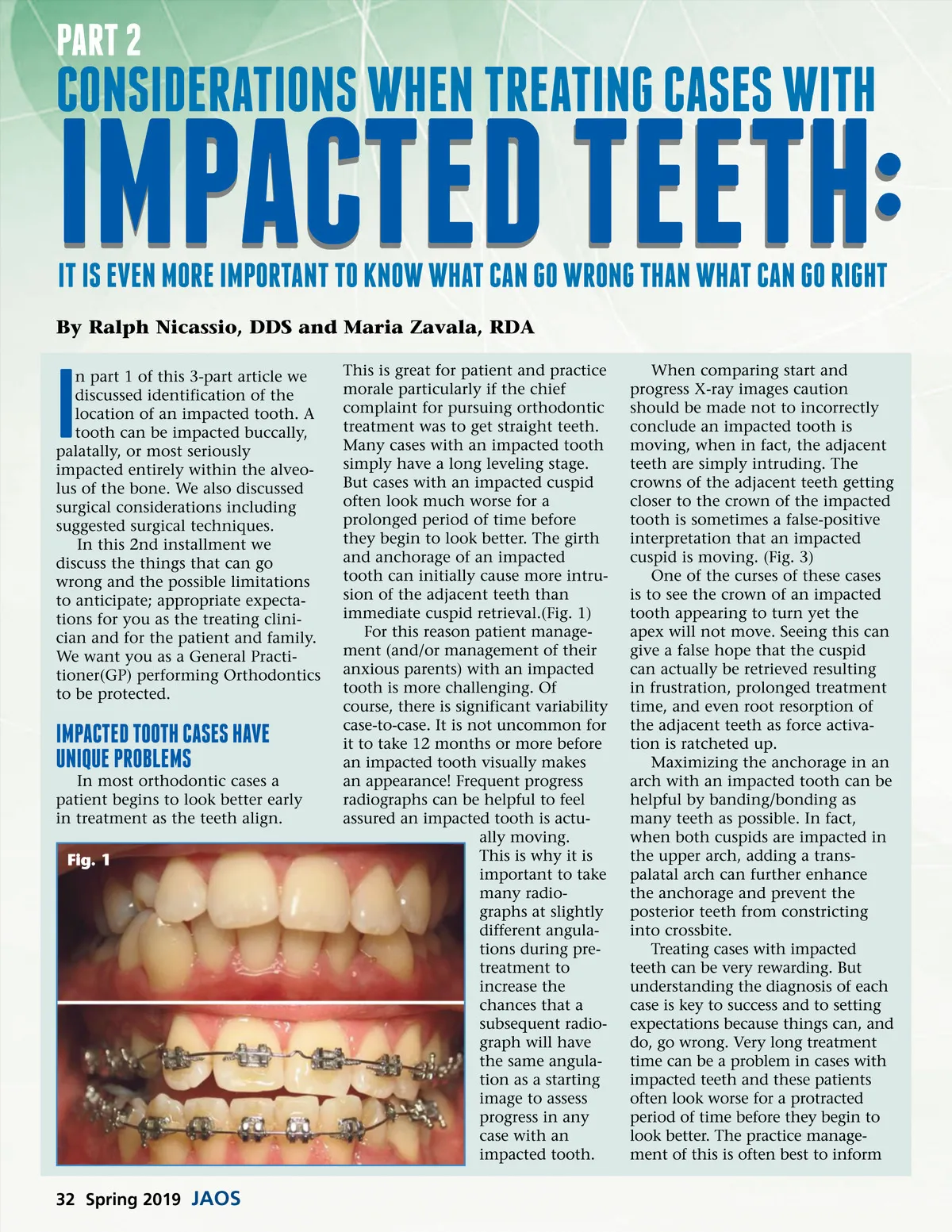
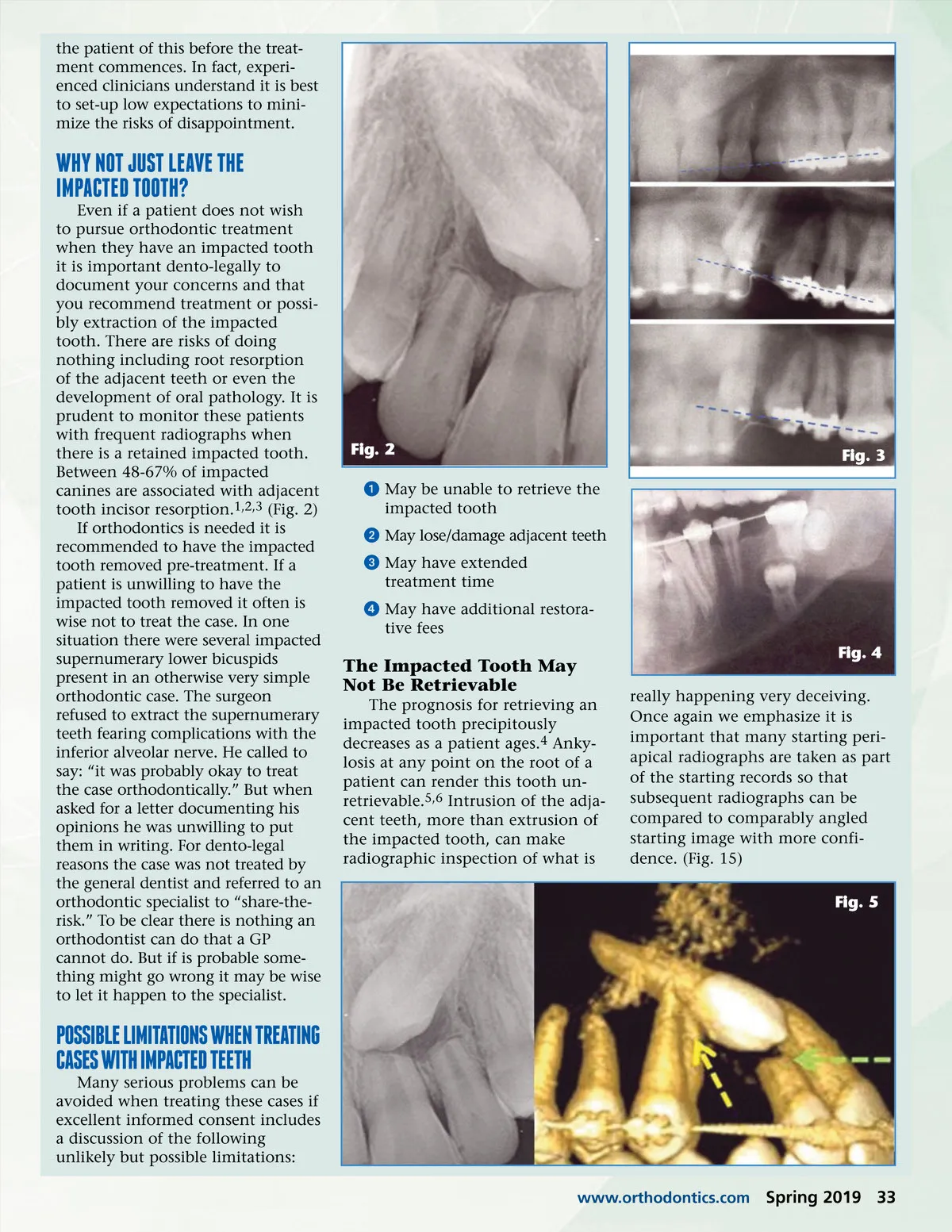
the patient of this before the treat-ment commences. In fact, experi-enced clinicians understand it is best to set-up low expectations to mini-mize the risks of disappointment. WhY not just leave the Impacted tooth? Even if a patient does not wish to pursue orthodontic treatment when they have an impacted tooth it is important dento-legally to document your concerns and that you recommend treatment or possi-bly extraction of the impacted tooth. There are risks of doing nothing including root resorption of the adjacent teeth or even the development of oral pathology. It is prudent to monitor these patients with frequent radiographs when there is a retained impacted tooth. Between 48-67% of impacted canines are associated with adjacent tooth incisor resorption. 1,2,3 (Fig. 2) If orthodontics is needed it is recommended to have the impacted tooth removed pre-treatment. If a patient is unwilling to have the impacted tooth removed it often is wise not to treat the case. In one situation there were several impacted supernumerary lower bicuspids present in an otherwise very simple orthodontic case. The surgeon refused to extract the supernumerary teeth fearing complications with the inferior alveolar nerve. He called to say: “it was probably okay to treat the case orthodontically.” But when asked for a letter documenting his opinions he was unwilling to put them in writing. For dento-legal reasons the case was not treated by the general dentist and referred to an orthodontic specialist to “share-the-risk.” To be clear there is nothing an orthodontist can do that a GP cannot do. But if is probable some-thing might go wrong it may be wise to let it happen to the specialist. Fig. 2 ᕡ May be unable to retrieve the impacted tooth ᕢ May lose/damage adjacent teeth ᕣ May have extended treatment time ᕤ May have additional restora-tive fees Fig. 3 The Impacted Tooth May Not Be Retrievable The prognosis for retrieving an impacted tooth precipitously decreases as a patient ages. 4 Anky-losis at any point on the root of a patient can render this tooth un-retrievable. 5,6 Intrusion of the adja-cent teeth, more than extrusion of the impacted tooth, can make radiographic inspection of what is Fig. 4 really happening very deceiving. Once again we emphasize it is important that many starting peri-apical radiographs are taken as part of the starting records so that subsequent radiographs can be compared to comparably angled starting image with more confi-dence. (Fig. 15) Fig. 5 possIble lImItatIons When treatIng cases WIth Impacted teeth Many serious problems can be avoided when treating these cases if excellent informed consent includes a discussion of the following unlikely but possible limitations: www.orthodontics.com Spring 2019 33
Journal of the American Orthodontic Society Spring 2019: Page 33