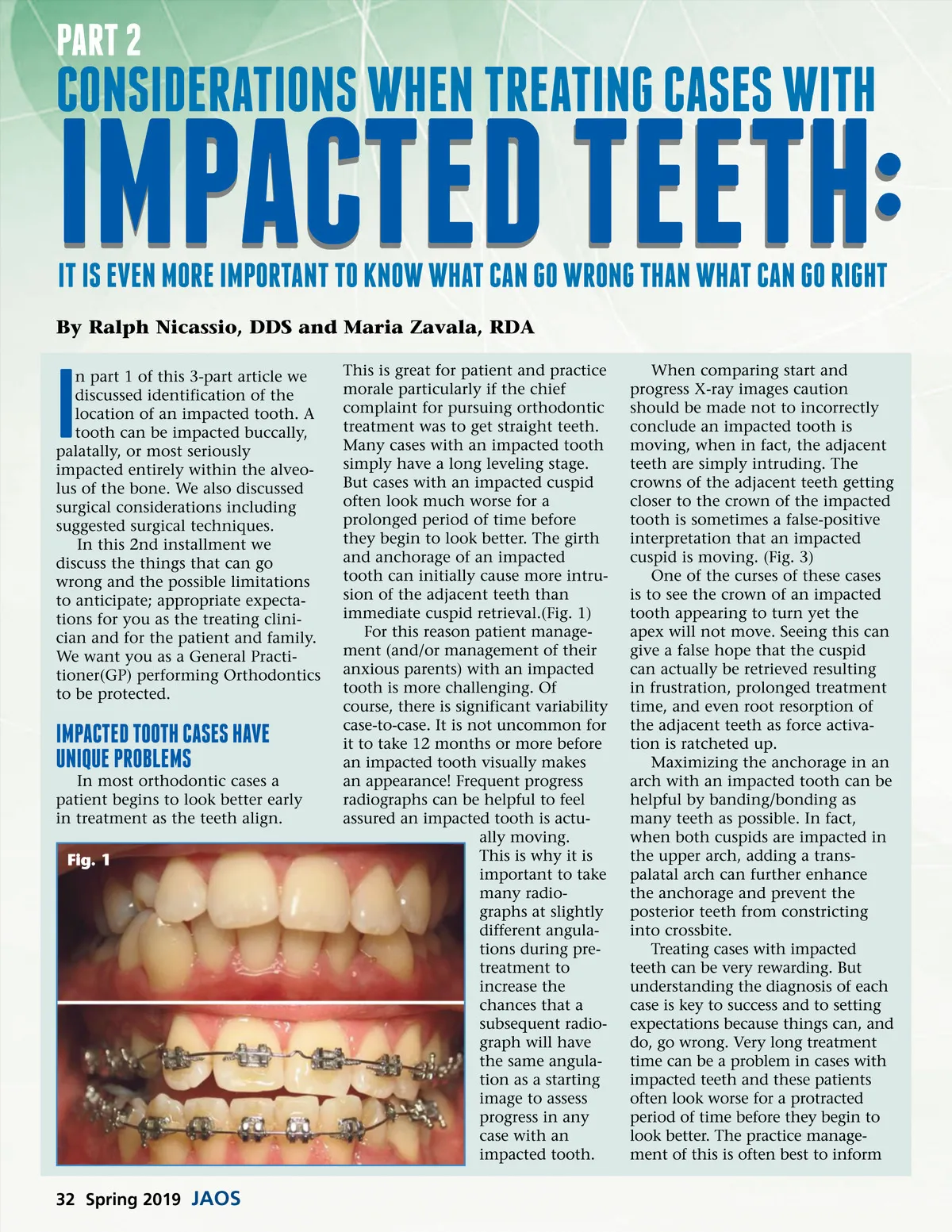
part 2 consIderatIons When treatIng cases WIth Impacted teeth: It Is even more Important to knoW What can go Wrong than What can go rIght This is great for patient and practice morale particularly if the chief complaint for pursuing orthodontic treatment was to get straight teeth. Many cases with an impacted tooth simply have a long leveling stage. But cases with an impacted cuspid often look much worse for a prolonged period of time before they begin to look better. The girth and anchorage of an impacted tooth can initially cause more intru-sion of the adjacent teeth than immediate cuspid retrieval.(Fig. 1) For this reason patient manage-ment (and/or management of their anxious parents) with an impacted tooth is more challenging. Of course, there is significant variability case-to-case. It is not uncommon for it to take 12 months or more before an impacted tooth visually makes an appearance! Frequent progress radiographs can be helpful to feel assured an impacted tooth is actu-ally moving. This is why it is important to take many radio-graphs at slightly different angula-tions during pre-treatment to increase the chances that a subsequent radio-graph will have the same angula-tion as a starting image to assess progress in any case with an impacted tooth. By Ralph Nicassio, DDS and Maria Zavala, RDA I n part 1 of this 3-part article we discussed identification of the location of an impacted tooth. A tooth can be impacted buccally, palatally, or most seriously impacted entirely within the alveo-lus of the bone. We also discussed surgical considerations including suggested surgical techniques. In this 2nd installment we discuss the things that can go wrong and the possible limitations to anticipate; appropriate expecta-tions for you as the treating clini-cian and for the patient and family. We want you as a General Practi-tioner(GP) performing Orthodontics to be protected. Impacted tooth cases have unIque problems In most orthodontic cases a patient begins to look better early in treatment as the teeth align. Fig. 1 When comparing start and progress X-ray images caution should be made not to incorrectly conclude an impacted tooth is moving, when in fact, the adjacent teeth are simply intruding. The crowns of the adjacent teeth getting closer to the crown of the impacted tooth is sometimes a false-positive interpretation that an impacted cuspid is moving. (Fig. 3) One of the curses of these cases is to see the crown of an impacted tooth appearing to turn yet the apex will not move. Seeing this can give a false hope that the cuspid can actually be retrieved resulting in frustration, prolonged treatment time, and even root resorption of the adjacent teeth as force activa-tion is ratcheted up. Maximizing the anchorage in an arch with an impacted tooth can be helpful by banding/bonding as many teeth as possible. In fact, when both cuspids are impacted in the upper arch, adding a trans-palatal arch can further enhance the anchorage and prevent the posterior teeth from constricting into crossbite. Treating cases with impacted teeth can be very rewarding. But understanding the diagnosis of each case is key to success and to setting expectations because things can, and do, go wrong. Very long treatment time can be a problem in cases with impacted teeth and these patients often look worse for a protracted period of time before they begin to look better. The practice manage-ment of this is often best to inform 32 Spring 2019 JAOS
Journal of the American Orthodontic Society Spring 2019: Page 32