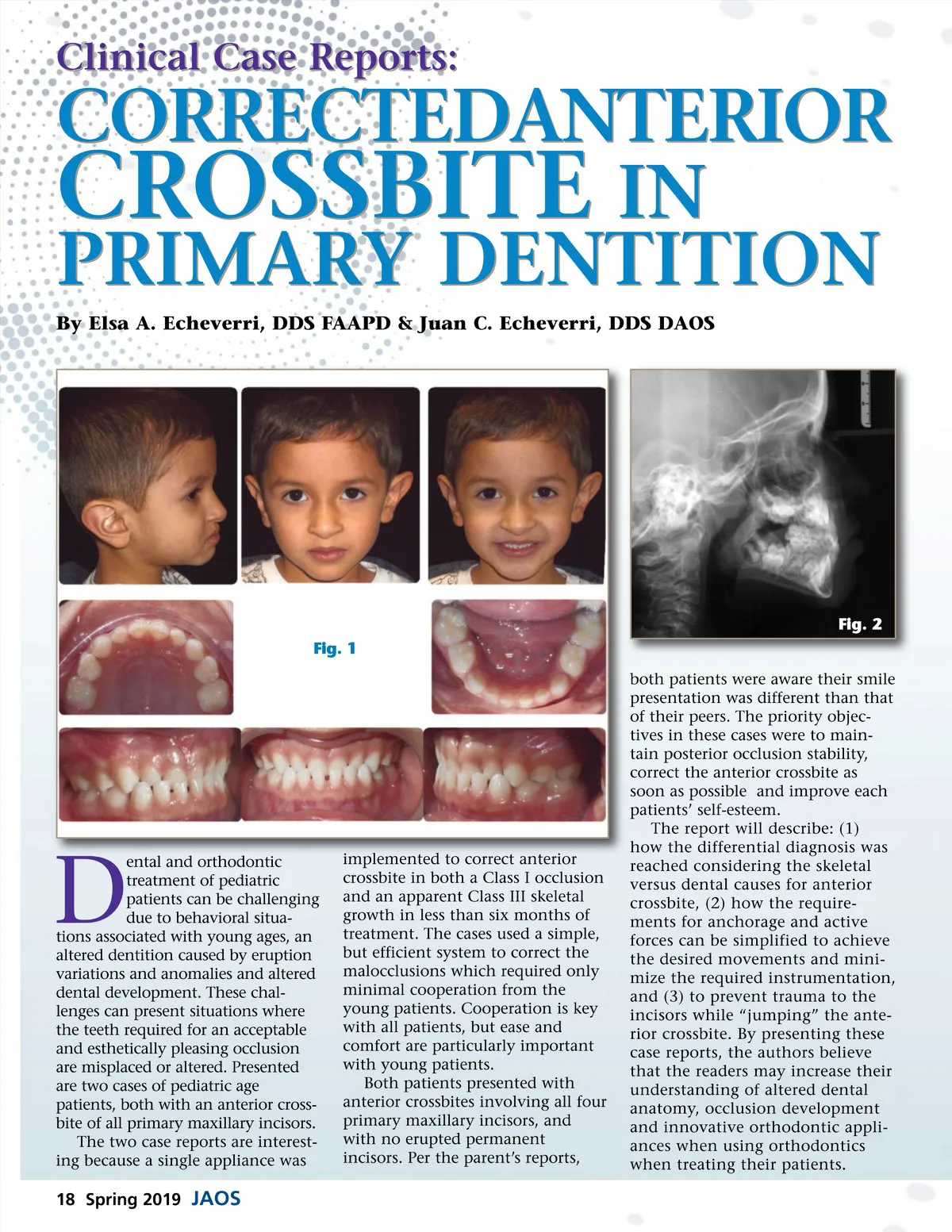
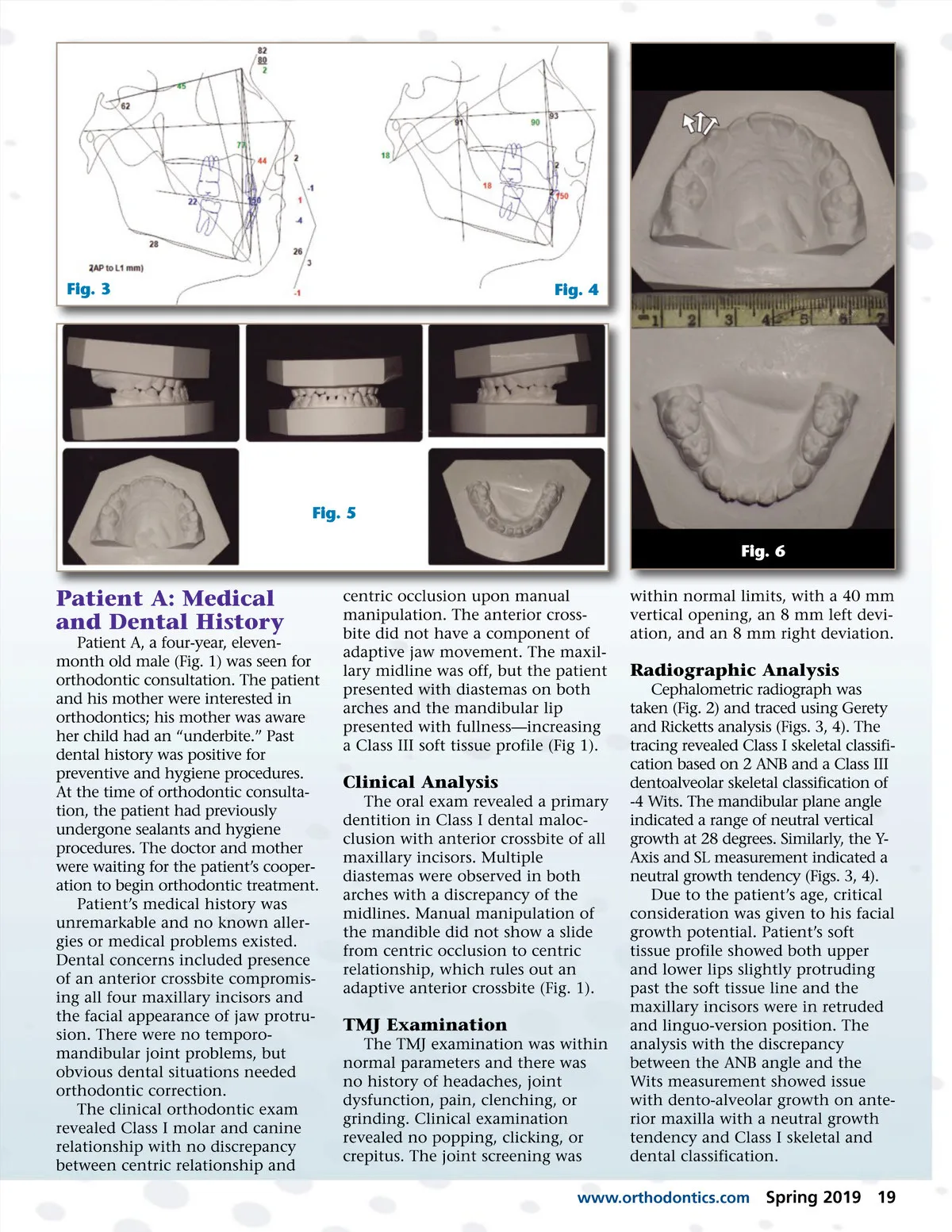
Fig. 3 Fig. 4 Fig. 5 Fig. 6 Patient A: Medical and Dental History Patient A, a four-year, eleven-month old male (Fig. 1) was seen for orthodontic consultation. The patient and his mother were interested in orthodontics; his mother was aware her child had an “underbite.” Past dental history was positive for preventive and hygiene procedures. At the time of orthodontic consulta-tion, the patient had previously undergone sealants and hygiene procedures. The doctor and mother were waiting for the patient’s cooper-ation to begin orthodontic treatment. Patient’s medical history was unremarkable and no known aller-gies or medical problems existed. Dental concerns included presence of an anterior crossbite compromis-ing all four maxillary incisors and the facial appearance of jaw protru-sion. There were no temporo-mandibular joint problems, but obvious dental situations needed orthodontic correction. The clinical orthodontic exam revealed Class I molar and canine relationship with no discrepancy between centric relationship and centric occlusion upon manual manipulation. The anterior cross-bite did not have a component of adaptive jaw movement. The maxil-lary midline was off, but the patient presented with diastemas on both arches and the mandibular lip presented with fullness—increasing a Class III soft tissue profile (Fig 1). within normal limits, with a 40 mm vertical opening, an 8 mm left devi-ation, and an 8 mm right deviation. Radiographic Analysis Cephalometric radiograph was taken (Fig. 2) and traced using Gerety and Ricketts analysis (Figs. 3, 4). The tracing revealed Class I skeletal classifi-cation based on 2 ANB and a Class III dentoalveolar skeletal classification of -4 Wits. The mandibular plane angle indicated a range of neutral vertical growth at 28 degrees. Similarly, the Y-Axis and SL measurement indicated a neutral growth tendency (Figs. 3, 4). Due to the patient’s age, critical consideration was given to his facial growth potential. Patient’s soft tissue profile showed both upper and lower lips slightly protruding past the soft tissue line and the maxillary incisors were in retruded and linguo-version position. The analysis with the discrepancy between the ANB angle and the Wits measurement showed issue with dento-alveolar growth on ante-rior maxilla with a neutral growth tendency and Class I skeletal and dental classification. Clinical Analysis The oral exam revealed a primary dentition in Class I dental maloc-clusion with anterior crossbite of all maxillary incisors. Multiple diastemas were observed in both arches with a discrepancy of the midlines. Manual manipulation of the mandible did not show a slide from centric occlusion to centric relationship, which rules out an adaptive anterior crossbite (Fig. 1). TMJ Examination The TMJ examination was within normal parameters and there was no history of headaches, joint dysfunction, pain, clenching, or grinding. Clinical examination revealed no popping, clicking, or crepitus. The joint screening was www.orthodontics.com Spring 2019 19
Journal of the American Orthodontic Society Spring 2019: Page 19