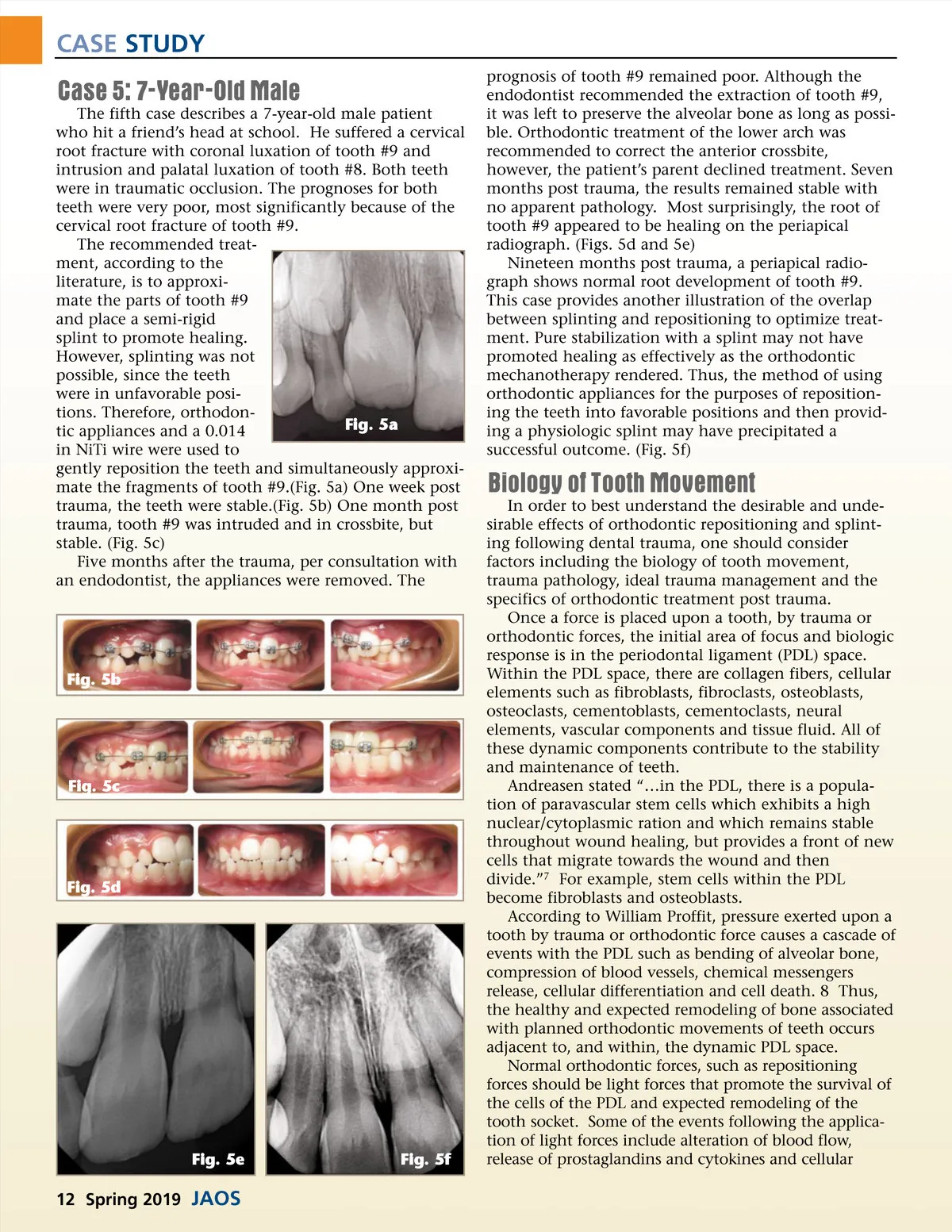
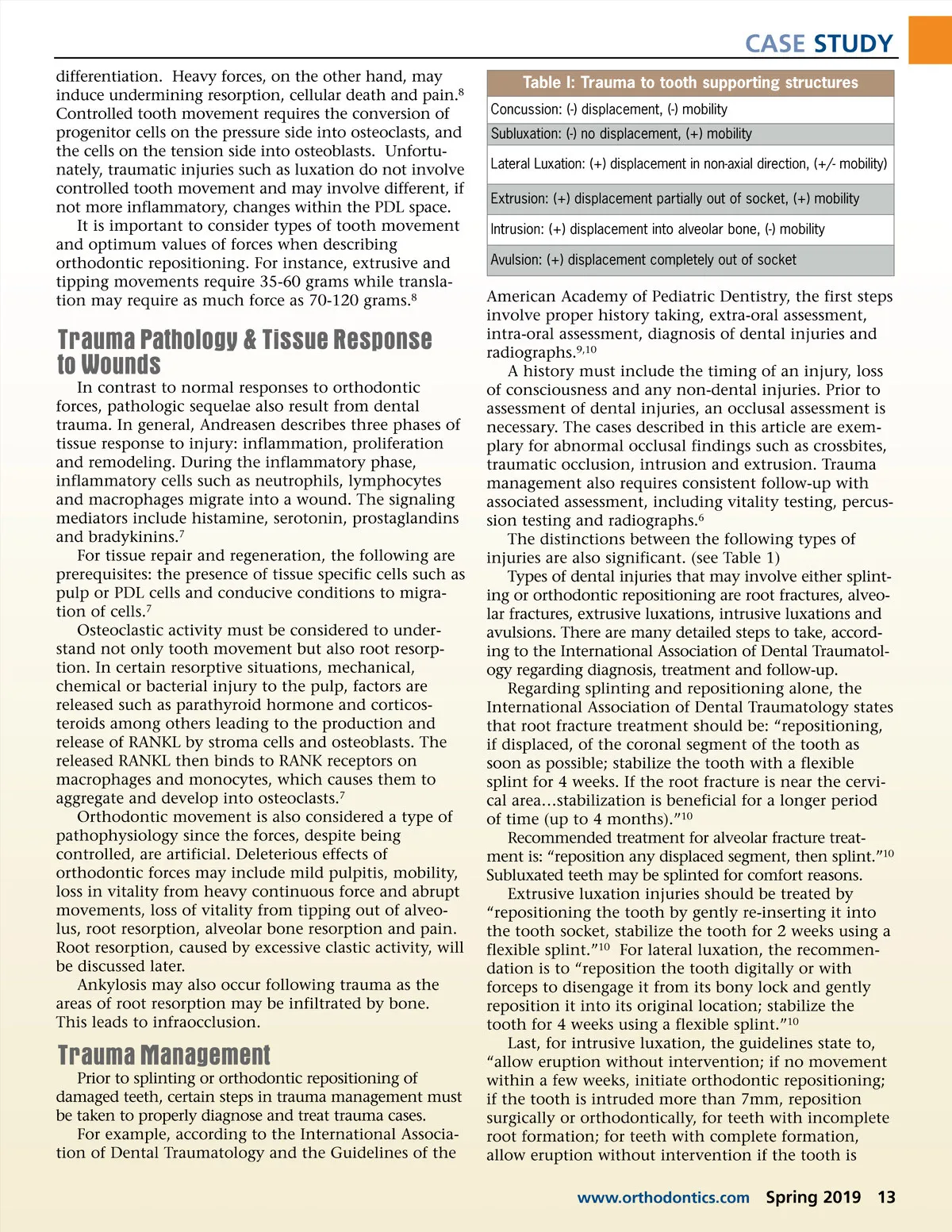
CASE STUDY Case 5: 7-Year-Old Male The fifth case describes a 7-year-old male patient who hit a friend’s head at school. He suffered a cervical root fracture with coronal luxation of tooth #9 and intrusion and palatal luxation of tooth #8. Both teeth were in traumatic occlusion. The prognoses for both teeth were very poor, most significantly because of the cervical root fracture of tooth #9. The recommended treat-ment, according to the literature, is to approxi-mate the parts of tooth #9 and place a semi-rigid splint to promote healing. However, splinting was not possible, since the teeth were in unfavorable posi-tions. Therefore, orthodon-Fig. 5a tic appliances and a 0.014 in NiTi wire were used to gently reposition the teeth and simultaneously approxi-mate the fragments of tooth #9.(Fig. 5a) One week post trauma, the teeth were stable.(Fig. 5b) One month post trauma, tooth #9 was intruded and in crossbite, but stable. (Fig. 5c) Five months after the trauma, per consultation with an endodontist, the appliances were removed. The prognosis of tooth #9 remained poor. Although the endodontist recommended the extraction of tooth #9, it was left to preserve the alveolar bone as long as possi-ble. Orthodontic treatment of the lower arch was recommended to correct the anterior crossbite, however, the patient’s parent declined treatment. Seven months post trauma, the results remained stable with no apparent pathology. Most surprisingly, the root of tooth #9 appeared to be healing on the periapical radiograph. (Figs. 5d and 5e) Nineteen months post trauma, a periapical radio-graph shows normal root development of tooth #9. This case provides another illustration of the overlap between splinting and repositioning to optimize treat-ment. Pure stabilization with a splint may not have promoted healing as effectively as the orthodontic mechanotherapy rendered. Thus, the method of using orthodontic appliances for the purposes of reposition-ing the teeth into favorable positions and then provid-ing a physiologic splint may have precipitated a successful outcome. (Fig. 5f) Biology of Tooth Movement In order to best understand the desirable and unde-sirable effects of orthodontic repositioning and splint-ing following dental trauma, one should consider factors including the biology of tooth movement, trauma pathology, ideal trauma management and the specifics of orthodontic treatment post trauma. Once a force is placed upon a tooth, by trauma or orthodontic forces, the initial area of focus and biologic response is in the periodontal ligament (PDL) space. Within the PDL space, there are collagen fibers, cellular elements such as fibroblasts, fibroclasts, osteoblasts, osteoclasts, cementoblasts, cementoclasts, neural elements, vascular components and tissue fluid. All of these dynamic components contribute to the stability and maintenance of teeth. Andreasen stated “…in the PDL, there is a popula-tion of paravascular stem cells which exhibits a high nuclear/cytoplasmic ration and which remains stable throughout wound healing, but provides a front of new cells that migrate towards the wound and then divide.” 7 For example, stem cells within the PDL become fibroblasts and osteoblasts. According to William Proffit, pressure exerted upon a tooth by trauma or orthodontic force causes a cascade of events with the PDL such as bending of alveolar bone, compression of blood vessels, chemical messengers release, cellular differentiation and cell death. 8 Thus, the healthy and expected remodeling of bone associated with planned orthodontic movements of teeth occurs adjacent to, and within, the dynamic PDL space. Normal orthodontic forces, such as repositioning forces should be light forces that promote the survival of the cells of the PDL and expected remodeling of the tooth socket. Some of the events following the applica-tion of light forces include alteration of blood flow, release of prostaglandins and cytokines and cellular Fig. 5b Fig. 5c Fig. 5d Fig. 5e Fig. 5f 12 Spring 2019 JAOS
Journal of the American Orthodontic Society Spring 2019: Page 12