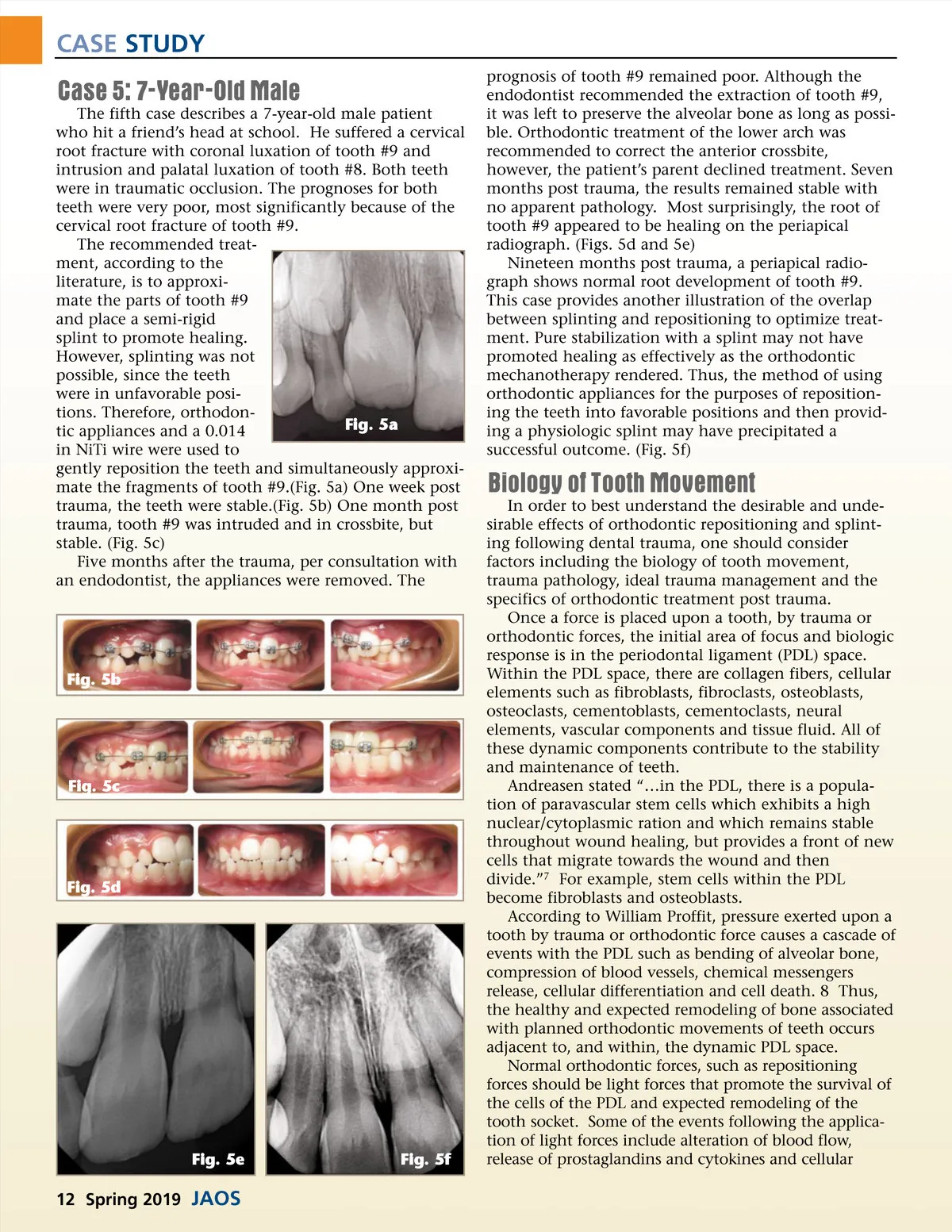
CASE STUDY differentiation. Heavy forces, on the other hand, may induce undermining resorption, cellular death and pain. 8 Controlled tooth movement requires the conversion of progenitor cells on the pressure side into osteoclasts, and the cells on the tension side into osteoblasts. Unfortu-nately, traumatic injuries such as luxation do not involve controlled tooth movement and may involve different, if not more inflammatory, changes within the PDL space. It is important to consider types of tooth movement and optimum values of forces when describing orthodontic repositioning. For instance, extrusive and tipping movements require 35-60 grams while transla-tion may require as much force as 70-120 grams. 8 Table I: Trauma to tooth supporting structures Concussion: (-) displacement, (-) mobility Subluxation: (-) no displacement, (+) mobility Lateral Luxation: (+) displacement in non-axial direction, (+/-mobility) Extrusion: (+) displacement partially out of socket, (+) mobility Intrusion: (+) displacement into alveolar bone, (-) mobility Avulsion: (+) displacement completely out of socket Trauma Pathology & Tissue Response to Wounds In contrast to normal responses to orthodontic forces, pathologic sequelae also result from dental trauma. In general, Andreasen describes three phases of tissue response to injury: inflammation, proliferation and remodeling. During the inflammatory phase, inflammatory cells such as neutrophils, lymphocytes and macrophages migrate into a wound. The signaling mediators include histamine, serotonin, prostaglandins and bradykinins. 7 For tissue repair and regeneration, the following are prerequisites: the presence of tissue specific cells such as pulp or PDL cells and conducive conditions to migra-tion of cells. 7 Osteoclastic activity must be considered to under-stand not only tooth movement but also root resorp-tion. In certain resorptive situations, mechanical, chemical or bacterial injury to the pulp, factors are released such as parathyroid hormone and corticos-teroids among others leading to the production and release of RANKL by stroma cells and osteoblasts. The released RANKL then binds to RANK receptors on macrophages and monocytes, which causes them to aggregate and develop into osteoclasts. 7 Orthodontic movement is also considered a type of pathophysiology since the forces, despite being controlled, are artificial. Deleterious effects of orthodontic forces may include mild pulpitis, mobility, loss in vitality from heavy continuous force and abrupt movements, loss of vitality from tipping out of alveo-lus, root resorption, alveolar bone resorption and pain. Root resorption, caused by excessive clastic activity, will be discussed later. Ankylosis may also occur following trauma as the areas of root resorption may be infiltrated by bone. This leads to infraocclusion. Trauma Management Prior to splinting or orthodontic repositioning of damaged teeth, certain steps in trauma management must be taken to properly diagnose and treat trauma cases. For example, according to the International Associa-tion of Dental Traumatology and the Guidelines of the American Academy of Pediatric Dentistry, the first steps involve proper history taking, extra-oral assessment, intra-oral assessment, diagnosis of dental injuries and radiographs. 9,10 A history must include the timing of an injury, loss of consciousness and any non-dental injuries. Prior to assessment of dental injuries, an occlusal assessment is necessary. The cases described in this article are exem-plary for abnormal occlusal findings such as crossbites, traumatic occlusion, intrusion and extrusion. Trauma management also requires consistent follow-up with associated assessment, including vitality testing, percus-sion testing and radiographs. 6 The distinctions between the following types of injuries are also significant. (see Table 1) Types of dental injuries that may involve either splint-ing or orthodontic repositioning are root fractures, alveo-lar fractures, extrusive luxations, intrusive luxations and avulsions. There are many detailed steps to take, accord-ing to the International Association of Dental Traumatol-ogy regarding diagnosis, treatment and follow-up. Regarding splinting and repositioning alone, the International Association of Dental Traumatology states that root fracture treatment should be: “repositioning, if displaced, of the coronal segment of the tooth as soon as possible; stabilize the tooth with a flexible splint for 4 weeks. If the root fracture is near the cervi-cal area…stabilization is beneficial for a longer period of time (up to 4 months).” 10 Recommended treatment for alveolar fracture treat-ment is: “reposition any displaced segment, then splint.” 10 Subluxated teeth may be splinted for comfort reasons. Extrusive luxation injuries should be treated by “repositioning the tooth by gently re-inserting it into the tooth socket, stabilize the tooth for 2 weeks using a flexible splint.” 10 For lateral luxation, the recommen-dation is to “reposition the tooth digitally or with forceps to disengage it from its bony lock and gently reposition it into its original location; stabilize the tooth for 4 weeks using a flexible splint.” 10 Last, for intrusive luxation, the guidelines state to, “allow eruption without intervention; if no movement within a few weeks, initiate orthodontic repositioning; if the tooth is intruded more than 7mm, reposition surgically or orthodontically, for teeth with incomplete root formation; for teeth with complete formation, allow eruption without intervention if the tooth is www.orthodontics.com Spring 2019 13
Journal of the American Orthodontic Society Spring 2019: Page 13