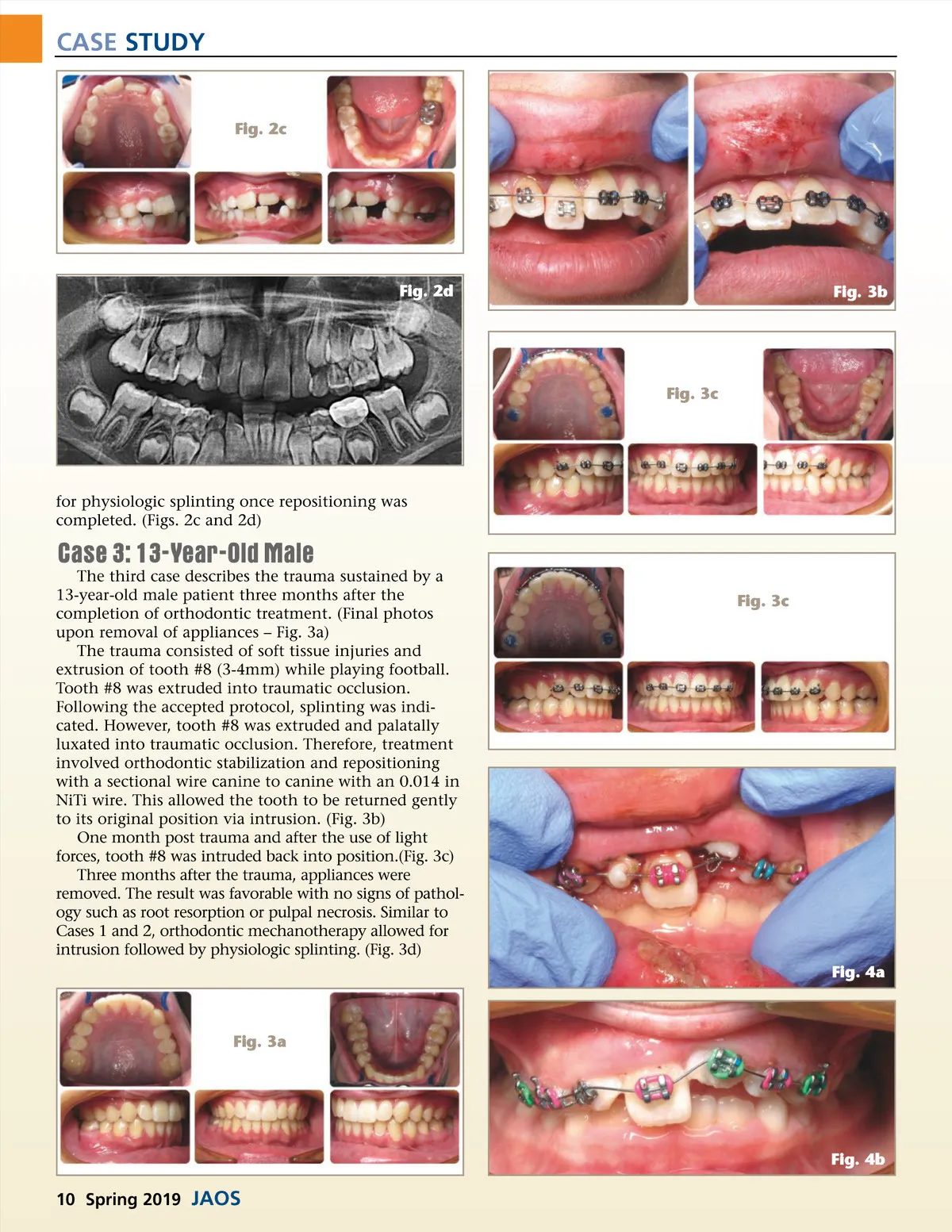
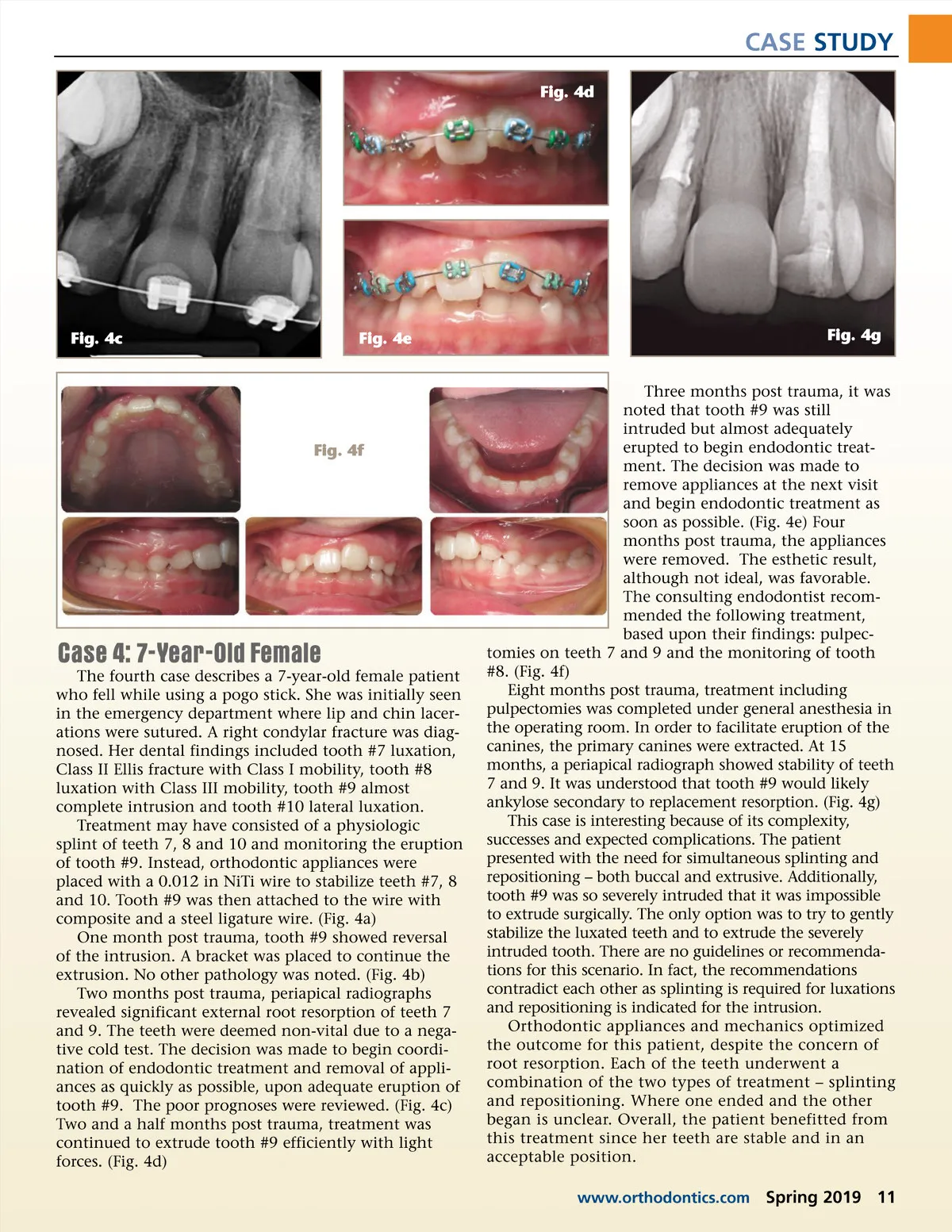
CASE STUDY Fig. 4d Fig. 4c Fig. 4e Fig. 4g Fig. 4f Case 4: 7-Year-Old Female The fourth case describes a 7-year-old female patient who fell while using a pogo stick. She was initially seen in the emergency department where lip and chin lacer-ations were sutured. A right condylar fracture was diag-nosed. Her dental findings included tooth #7 luxation, Class II Ellis fracture with Class I mobility, tooth #8 luxation with Class III mobility, tooth #9 almost complete intrusion and tooth #10 lateral luxation. Treatment may have consisted of a physiologic splint of teeth 7, 8 and 10 and monitoring the eruption of tooth #9. Instead, orthodontic appliances were placed with a 0.012 in NiTi wire to stabilize teeth #7, 8 and 10. Tooth #9 was then attached to the wire with composite and a steel ligature wire. (Fig. 4a) One month post trauma, tooth #9 showed reversal of the intrusion. A bracket was placed to continue the extrusion. No other pathology was noted. (Fig. 4b) Two months post trauma, periapical radiographs revealed significant external root resorption of teeth 7 and 9. The teeth were deemed non-vital due to a nega-tive cold test. The decision was made to begin coordi-nation of endodontic treatment and removal of appli-ances as quickly as possible, upon adequate eruption of tooth #9. The poor prognoses were reviewed. (Fig. 4c) Two and a half months post trauma, treatment was continued to extrude tooth #9 efficiently with light forces. (Fig. 4d) Three months post trauma, it was noted that tooth #9 was still intruded but almost adequately erupted to begin endodontic treat-ment. The decision was made to remove appliances at the next visit and begin endodontic treatment as soon as possible. (Fig. 4e) Four months post trauma, the appliances were removed. The esthetic result, although not ideal, was favorable. The consulting endodontist recom-mended the following treatment, based upon their findings: pulpec-tomies on teeth 7 and 9 and the monitoring of tooth #8. (Fig. 4f) Eight months post trauma, treatment including pulpectomies was completed under general anesthesia in the operating room. In order to facilitate eruption of the canines, the primary canines were extracted. At 15 months, a periapical radiograph showed stability of teeth 7 and 9. It was understood that tooth #9 would likely ankylose secondary to replacement resorption. (Fig. 4g) This case is interesting because of its complexity, successes and expected complications. The patient presented with the need for simultaneous splinting and repositioning – both buccal and extrusive. Additionally, tooth #9 was so severely intruded that it was impossible to extrude surgically. The only option was to try to gently stabilize the luxated teeth and to extrude the severely intruded tooth. There are no guidelines or recommenda-tions for this scenario. In fact, the recommendations contradict each other as splinting is required for luxations and repositioning is indicated for the intrusion. Orthodontic appliances and mechanics optimized the outcome for this patient, despite the concern of root resorption. Each of the teeth underwent a combination of the two types of treatment – splinting and repositioning. Where one ended and the other began is unclear. Overall, the patient benefitted from this treatment since her teeth are stable and in an acceptable position. www.orthodontics.com Spring 2019 11
Journal of the American Orthodontic Society Spring 2019: Page 11