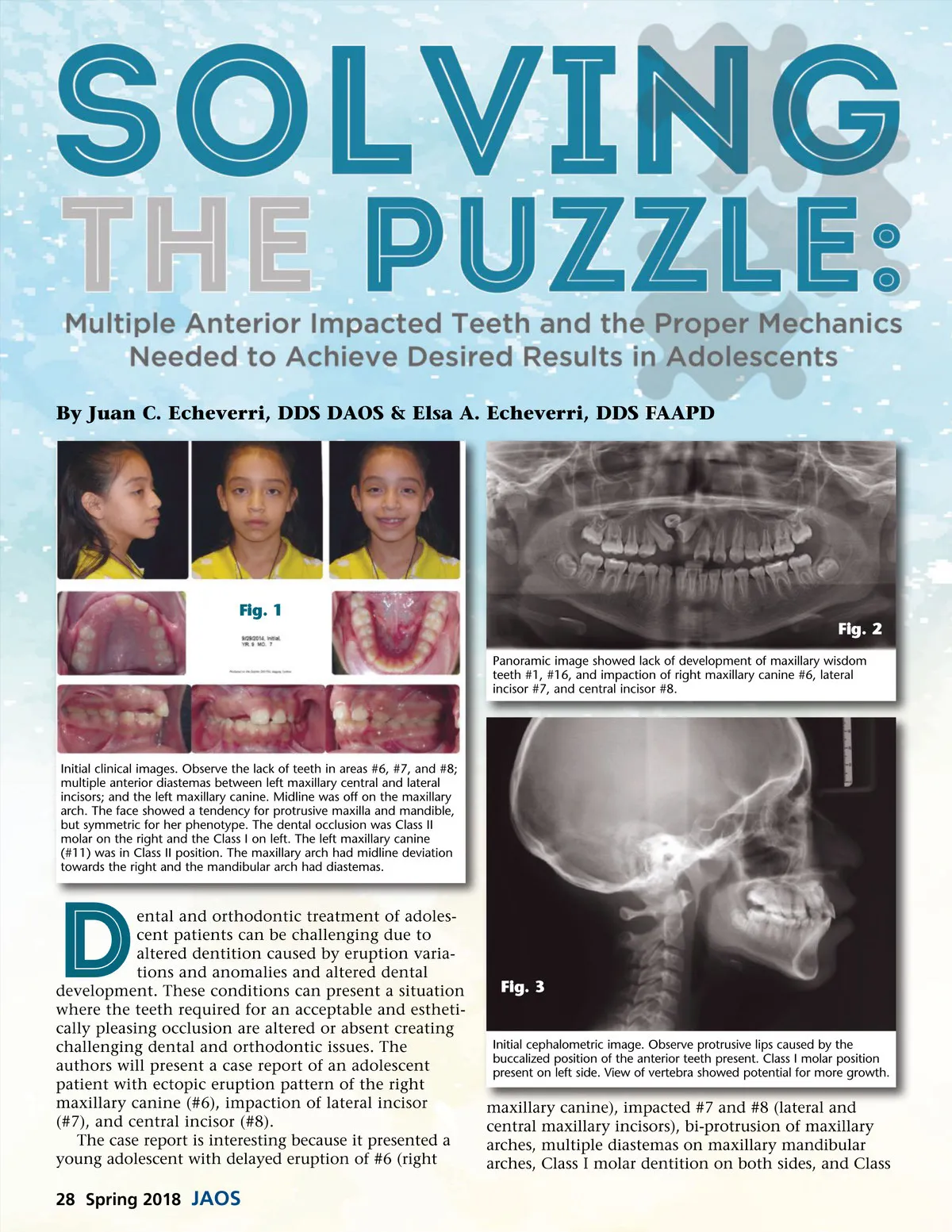
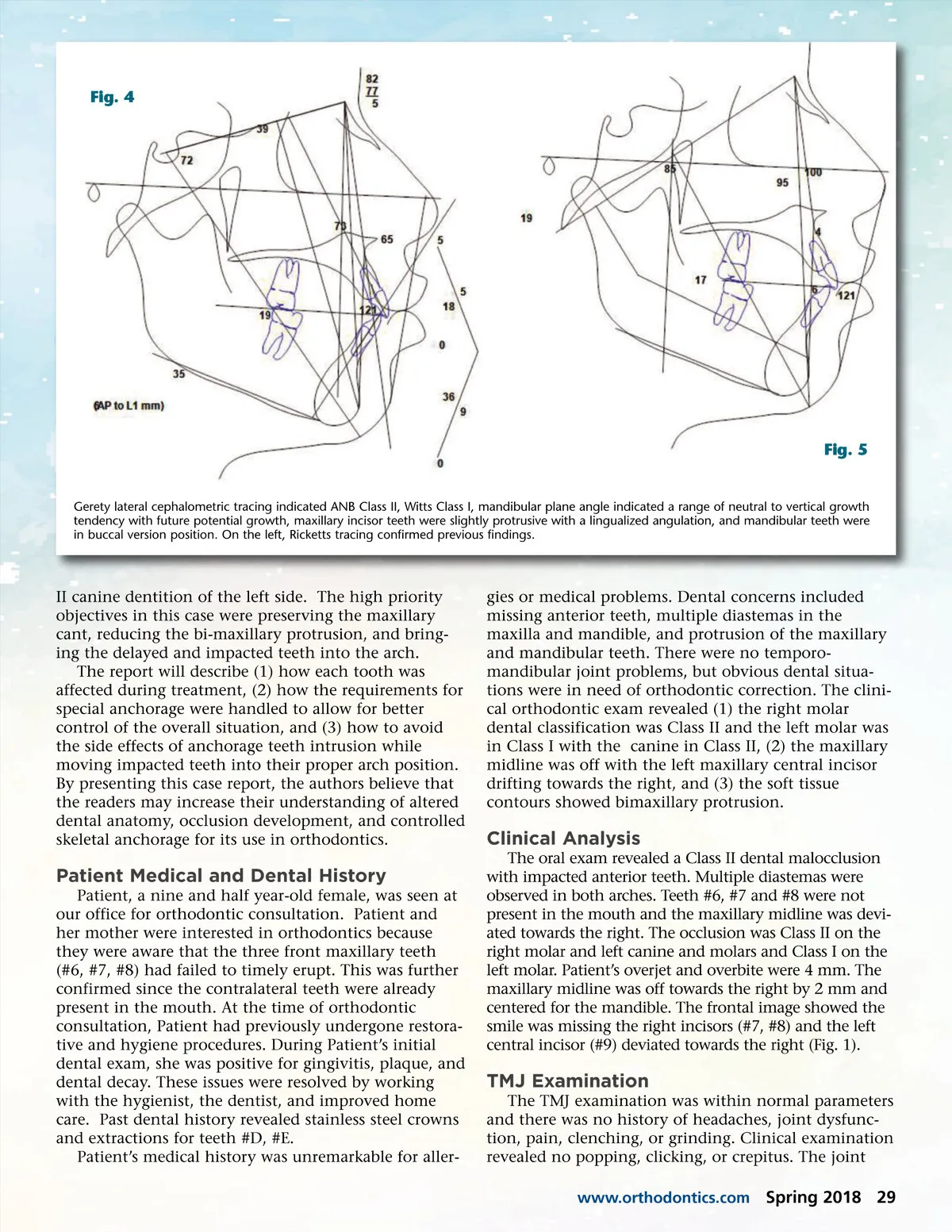
Fig. 4 Fig. 5 Gerety lateral cephalometric tracing indicated ANB Class II, Witts Class I, mandibular plane angle indicated a range of neutral to vertical growth tendency with future potential growth, maxillary incisor teeth were slightly protrusive with a lingualized angulation, and mandibular teeth were in buccal version position. On the left, Ricketts tracing confirmed previous findings. II canine dentition of the left side. The high priority objectives in this case were preserving the maxillary cant, reducing the bi-maxillary protrusion, and bring-ing the delayed and impacted teeth into the arch. The report will describe (1) how each tooth was affected during treatment, (2) how the requirements for special anchorage were handled to allow for better control of the overall situation, and (3) how to avoid the side effects of anchorage teeth intrusion while moving impacted teeth into their proper arch position. By presenting this case report, the authors believe that the readers may increase their understanding of altered dental anatomy, occlusion development, and controlled skeletal anchorage for its use in orthodontics. gies or medical problems. Dental concerns included missing anterior teeth, multiple diastemas in the maxilla and mandible, and protrusion of the maxillary and mandibular teeth. There were no temporo-mandibular joint problems, but obvious dental situa-tions were in need of orthodontic correction. The clini-cal orthodontic exam revealed (1) the right molar dental classification was Class II and the left molar was in Class I with the canine in Class II, (2) the maxillary midline was off with the left maxillary central incisor drifting towards the right, and (3) the soft tissue contours showed bimaxillary protrusion. Clinical Analysis The oral exam revealed a Class II dental malocclusion with impacted anterior teeth. Multiple diastemas were observed in both arches. Teeth #6, #7 and #8 were not present in the mouth and the maxillary midline was devi-ated towards the right. The occlusion was Class II on the right molar and left canine and molars and Class I on the left molar. Patient’s overjet and overbite were 4 mm. The maxillary midline was off towards the right by 2 mm and centered for the mandible. The frontal image showed the smile was missing the right incisors (#7, #8) and the left central incisor (#9) deviated towards the right (Fig. 1). Patient Medical and Dental History Patient, a nine and half year-old female, was seen at our office for orthodontic consultation. Patient and her mother were interested in orthodontics because they were aware that the three front maxillary teeth (#6, #7, #8) had failed to timely erupt. This was further confirmed since the contralateral teeth were already present in the mouth. At the time of orthodontic consultation, Patient had previously undergone restora-tive and hygiene procedures. During Patient’s initial dental exam, she was positive for gingivitis, plaque, and dental decay. These issues were resolved by working with the hygienist, the dentist, and improved home care. Past dental history revealed stainless steel crowns and extractions for teeth #D, #E. Patient’s medical history was unremarkable for aller-TMJ Examination The TMJ examination was within normal parameters and there was no history of headaches, joint dysfunc-tion, pain, clenching, or grinding. Clinical examination revealed no popping, clicking, or crepitus. The joint www.orthodontics.com Spring 2018 29
Journal of the American Orthodontic Society Spring 2018: Page 29