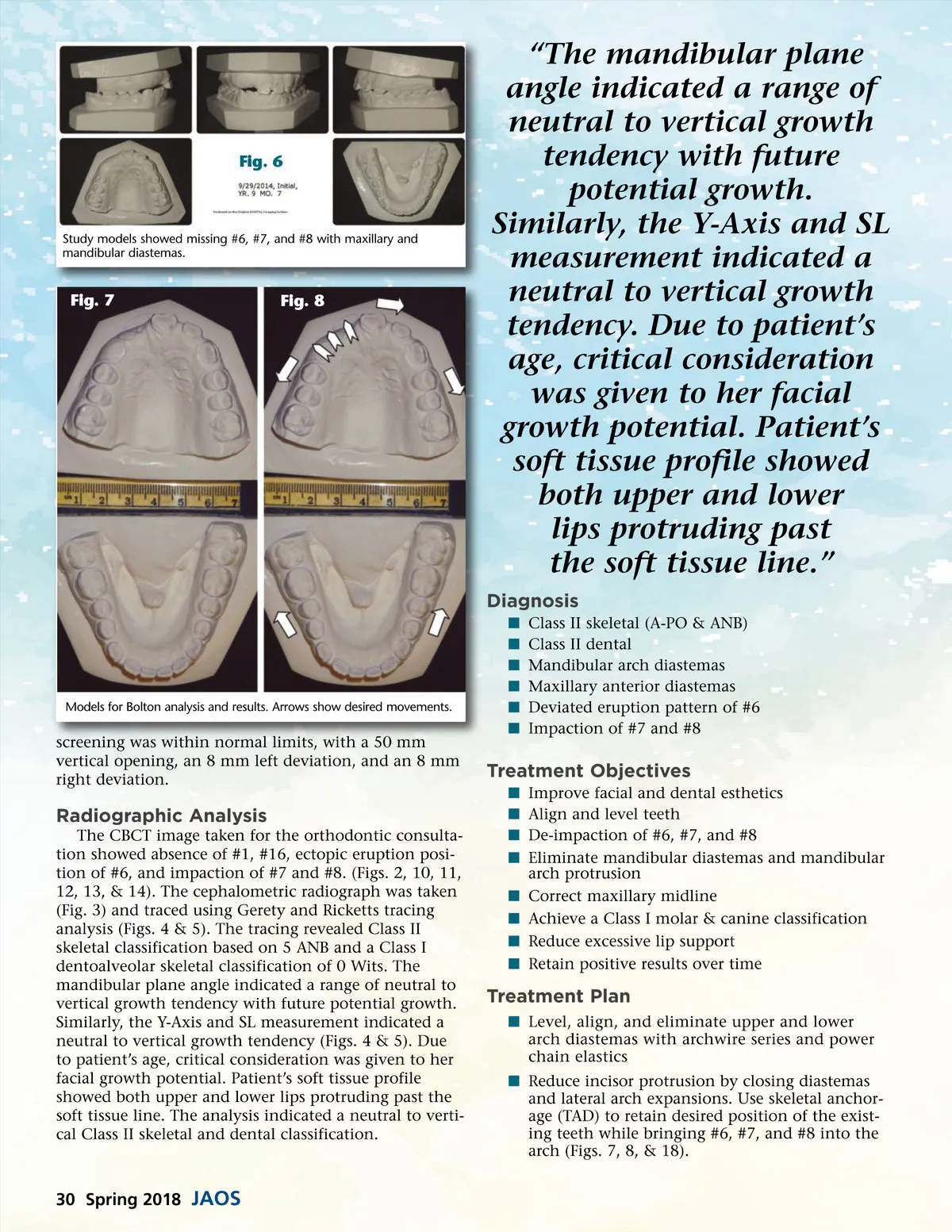
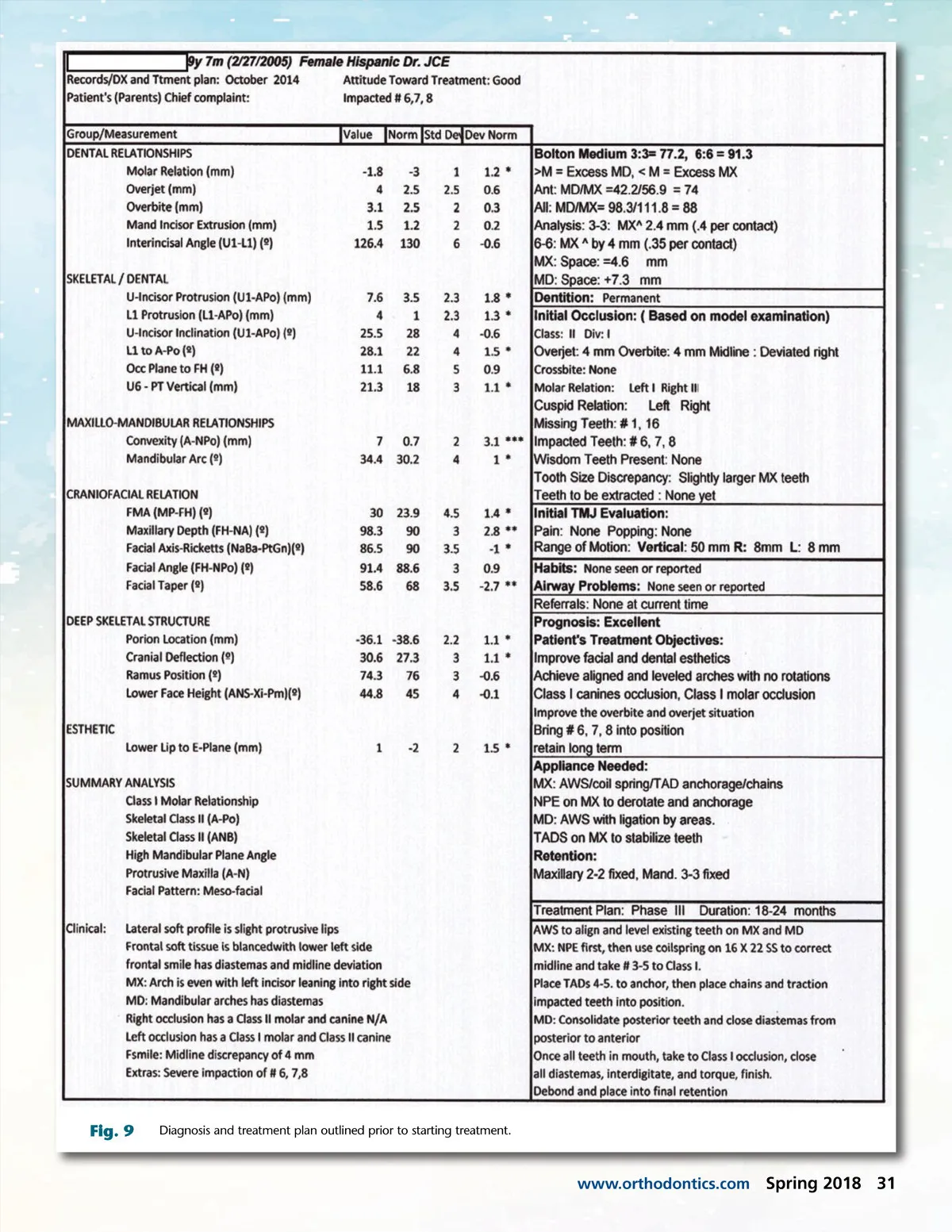
Fig. 6 Study models showed missing #6, #7, and #8 with maxillary and mandibular diastemas. Fig. 7 Fig. 8 “The mandibular plane angle indicated a range of neutral to vertical growth tendency with future potential growth. Similarly, the Y-Axis and SL measurement indicated a neutral to vertical growth tendency. Due to patient’s age, critical consideration was given to her facial growth potential. Patient’s soft tissue profile showed both upper and lower lips protruding past the soft tissue line.” Diagnosis í í í í í í Class II skeletal (A-PO & ANB) Class II dental Mandibular arch diastemas Maxillary anterior diastemas Deviated eruption pattern of #6 Impaction of #7 and #8 Models for Bolton analysis and results. Arrows show desired movements. screening was within normal limits, with a 50 mm vertical opening, an 8 mm left deviation, and an 8 mm right deviation. Treatment Objectives í í í í í í í í Improve facial and dental esthetics Align and level teeth De-impaction of #6, #7, and #8 Eliminate mandibular diastemas and mandibular arch protrusion Correct maxillary midline Achieve a Class I molar & canine classification Reduce excessive lip support Retain positive results over time Radiographic Analysis The CBCT image taken for the orthodontic consulta-tion showed absence of #1, #16, ectopic eruption posi-tion of #6, and impaction of #7 and #8. (Figs. 2, 10, 11, 12, 13, & 14). The cephalometric radiograph was taken (Fig. 3) and traced using Gerety and Ricketts tracing analysis (Figs. 4 & 5). The tracing revealed Class II skeletal classification based on 5 ANB and a Class I dentoalveolar skeletal classification of 0 Wits. The mandibular plane angle indicated a range of neutral to vertical growth tendency with future potential growth. Similarly, the Y-Axis and SL measurement indicated a neutral to vertical growth tendency (Figs. 4 & 5). Due to patient’s age, critical consideration was given to her facial growth potential. Patient’s soft tissue profile showed both upper and lower lips protruding past the soft tissue line. The analysis indicated a neutral to verti-cal Class II skeletal and dental classification. Treatment Plan í Level, align, and eliminate upper and lower arch diastemas with archwire series and power chain elastics í Reduce incisor protrusion by closing diastemas and lateral arch expansions. Use skeletal anchor-age (TAD) to retain desired position of the exist-ing teeth while bringing #6, #7, and #8 into the arch (Figs. 7, 8, & 18). 30 Spring 2018 JAOS
Journal of the American Orthodontic Society Spring 2018: Page 30